Positive Health Online
Your Country

![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
Thermography in Dental Practice
by Dr Graeme Munro-Hall and Dr Lilian Munro-Hall(more info)
listed in dentistry, originally published in issue 202 - January 2013
Thermography is not new in dentistry. The first articles about thermography in dentistry appeared in the 1970s but it has never been taken up as a useful adjunctive diagnostic tool in either hospital or general practice settings. A thermography camera picks up infrared heat emissions and displays the result in a coloured picture where each colour represents a certain temperature.

Patient with hot right cheek
Caption: Thermal image showing hotter area on right side of face. This could be a sinus infection or a dentally related infection or a skin infection. Controlling the variables eliminates errors such as sitting near a heat source, rubbing the cheek etc.
Thermography compares the right side with left side of the face. The reason for the difference in temperature now has to be investigated. It has always created controversy in the academic world and has not been generally accepted as either accurate or useful. However, recent advances in the technology of thermal cameras and their software have, in our view, rendered these objections invalid. Provided the variables are controlled as discussed below, we have found thermography to be both accurate and useful.
We were after a screening tool to look for NICO’s, (Neuralgia Inducing Cavitational Osteitis), cavitation infections and inflammations in the head and neck associated with infections.[1, 2]
X-Rays do not always show such pathologies, and ultrasound devices such as the Cavitat, although accurate, take time, are expensive and intrusive. We have used the Cavitat for ten years and have found it to be excellent at picking up structural defects such as chronic cavitation infections in the bone, but as a screening aid it has serious limitations.[3]
Thermography picks up physiological and functional changes in tissues that occur before any structural changes can be seen. Thermography could be used to screen all patients; it can pick up pathological changes before any of the conventional diagnostic aids such as radiographs and ultrasound.
Thermography is non invasive, no ionising radiation is used, no physical contact is made with the patient and it can be used to detect inflammation and as a monitoring tool post treatment. These are distinct advantages over all other diagnostic systems. Thermography can only show radiant heat pictures with increased heat meaning inflammation. This can detect infection in the tissues is picked up earlier than with any other diagnostic aid as it shows physiological rather than physical or structural changes. Physiological changes always occur before physical changes.
In humans, radiation is the primary source of heat transfer and exchange to the environment. The infrared spectrum is from 0.8 microns to 25 microns. Human skin peak emission occurs at 9 microns and has an emissivity of 0.98 which is close to the emissivity of a black body at 1.0, so skin is close to the ideal emitter of infrared radiation. This makes thermography a good tool to use in the diagnosis and monitoring of pathologies.
Thermography systems specific for the whole body are around the £30,000 mark and as we were only interested in the head and neck we decided on the FLIR B335 made in Sweden at around one third of the cost.

FLIR B335 thermal camera
This camera was chosen as it met the specifications of the medical thermography systems and has been used in Veterinary medicine for some years. The camera picks up in the 7.5 to 13 microns range with a thermal sensitivity of 0.05°C at 30.0°C and has a high resolution. The temperature range of the FLIR B335 was -20°C to 120°C. The standard lens was sufficient for our purpose and the FLIR software package was excellent in all aspects. We have had the camera for 18 months now and it has performed well. The learning curve, though steep, was manageable.
Cheaper hand held cameras are available from the Far East and also from FLIR, but at a lower specification. In time technological advances may allow such cameras to be used in practice. The camera has a touch screen, and images can be stored directly onto a computer or to an SD card. Training was non existent, as no-one has used it for dental applications before, so we learnt as we went along.
Variables have to be controlled for accuracy. Stefan-Boltzman Law states that energy transfer from a body to the environment is dependant on the temperature difference between the two, so a controlled environment for taking the pictures is essential.
The imaging room is ideally about 10 ft square, no reflective surfaces, temperature controlled between 18°C & 22°C, no draughts and no extraneous heat sources. The patient must be acclimatized for 20 minutes beforehand and attention paid to pimples, razor nicks, sunburn, heavy make-up and especially touching the face with fingers. If a hand is briefly pressed on a surface the heat picture is discernable for several minutes after the hand is removed. Scratching a nose will distort the image for several minutes afterwards.
Ideally the camera should be on a tripod for stability and focusing is absolutely critical. Any slight movement renders the image useless. Likewise the focus has to be absolutely spot on. We have found 80-100 cm distance is ideal for dental purposes using the standard lens. We take a front view including the neck and a left and right profile as well. This way we can evaluate trigger points and any carotid occlusion and thyroid abnormalities as well as dental related areas.
Once the pictures are taken we transfer them from the SD card to a computer for evaluation. Once on the computer, different views are possible, enlargements, specific areas, line gradients, spot measurements etc. and the data is saved. This does take time, at least double the time needed to take and evaluate a digital OPG. An image is immediately available on the camera but accurate evaluation can only take place using a computer.
Men are hotter than women interestingly enough from a thermography point of view, but absolute values are not used. Thermography uses comparative values. One side is compared to the other side and to adjacent tissues. In the head and neck, temperature differences up to 0.25ºC are regarded as normal. Up to 0.35ºC difference is equivocal, greater than 0.35 is a hot area, i.e. inflamed. Any area lower than 0.35ºC is regarded as a cold area.
In peripheral nerve mediated pain and mental or ID nerve damage the temperature is 0.5ºC lower than the contra lateral side.
In TMD syndrome, if the differential between the right and left TMJs is 0.4ºC or greater, this indicates a TMJ problem. It is an ideal way of monitoring progress in treating TMD. We have found this to be very valuable in practice.[4, 5] It is quick, easy and accurate.
Thermography has a history of early cancer detection; in breast cancer it is more reliable than Mammograms and picks up pathology some three years earlier than mammograms without using ionising radiation.[6] We have detected the presence of cancer in of two patients using thermography in the last year which was later confirmed.
Increased heat means inflammation in an area. Dentally this could be in the maxillary sinus, active gingival infection, abscessed or necrotic teeth, root filled teeth, cavitation infection, retained roots, third molar extraction sites and so on.
Thermography is an adjunctive tool and cannot be used without the use of an Orthopantomogram (OPG) picture to localize the area of concern. It is impossible to localize any area to a specific tooth with thermography. What we can see is the approximate position of inflammation and use visual examination and radiographs to find the exact location.
When used as a screening device alongside an OPG picture, it can tell us what patients will need further investigation using an ultrasound Cavitat scan or whether a particular tooth needs to be tested for toxicity. We have found that when the OPG shows nothing but there is a hot area, a Komstar toxicity test (www.komstar.ch ) will find a dead or dying symptomless tooth that otherwise would have been overlooked. Thermography also has shown pathology in implants that might have remained undetected and would be a useful tool in assessing implant sites before and after insertion of the implant.
Our particular practice philosophy is to remove all toxic foci from the mouth to restore and maintain good health. Infections are to be eliminated and thermography has helped in identifying infected areas to be treated that might otherwise have been missed. By picking up pathology early, before structural changes have occurred, this can actually reduce trauma to the patient. Sometimes we can reverse a condition before the situation becomes too late; this is true in occlusally related problems for example.
In myofascial pain, trigger points in neck and back muscles that refer pain to facial muscles can be picked up and the appropriate treatment prescribed. It is easy and simple to monitor progress using thermography to detect the trigger points.[7]
Cancers are always hot, hence use of thermography in their detection. We have had many patients with cancer and we have found that every single one has an infective dental pathology present. Furthermore, the side of dental pathology is the same side of the body that the cancer is primarily situated. This is not to say that all dental infections lead to cancer; it is just an observation we have made. However, others have noticed this connection as well, such as Dr Simon Yu in the USA, Dr Mostovy in Canada and the North Carolina Institute of Technology.
The latter go further and claim that breast cancer in particular is always associated with dental pathology and whatever side the infection is in the mouth is the side of the start of the cancer. The truth of this assertion may be open to question but hopefully more research in this area will be forthcoming.
.jpg)
Thermal Image Patient A
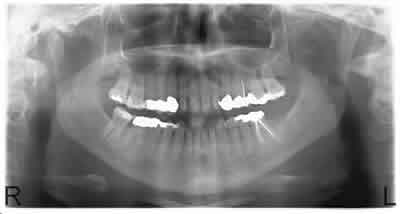
OPG radiograph patient A
Patient A
Thermal image showed hotter area on the left side of both upper and lower jaws. The patient had no symptoms apparent. Further examination revealed a root filled tooth, 25, which was highly toxic on Komstar testing and a cavitation infection where the upper left eight had been extracted 20+ years previously. The cavitation had destroyed the bone into the maxillary sinus. This would explain the large area seen on the thermal image. The lower image shows one hot spot that was in the areas of the root filled lower left first molar. Apical pathology can be easily seen on the OPG on this tooth and there is a cavitation infection in the bone immediately behind this tooth, which is hinted at on the OPG.
The patient must be informed about the pathology discovered and make her own mind up whether these areas are to be treated. Treatment would consist of opening and cleaning out the cavitation infection and extracting the two root filled teeth, properly cleaning out the sockets at the same time. Chronic infections are deleterious to the overall general health and nowhere else in the body other than the mouth would such infections be allowed to remain untreated.
.jpg)
Thermal image patient B

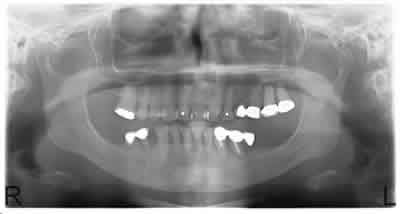
OPG radiograph patient B
Patient B
Diagnosed with metastasising bilateral breast cancer. The thermal image showed increased temperature on the right side associated with the lower jaw. The OPG showed pathology associated with the lower right eight and the molars on both jaws on the left .The Cavitat scan confirmed the presence of these infections as well as a cavitation infection in the bone where the second and first molars had been extracted 15 years previously. One cancerous area was an open wound and painful. After the dental treatment, the wound closed and the pain dissipated. The patient had declined all conventional cancer treatment for many years; whether such dental intervention will help her condition is unknown as yet.
.jpg)
Medical palette view patient C
.jpg)
Conventional thermal image patient C
OPG radiograph patient C
Patient C
Also a breast cancer patient, left breast. Once again she had declined all conventional treatment. Her Thermal image showed increase of temperature on the left side of the face. With a computer the picture can be viewed by different palettes in the software. Here are the normal view and the medical palette view of the same picture. Within the various palettes specific areas can be enhanced and magnified to aid diagnosis.
The OPG shows massive infectious destruction on the upper left and on the lower jaw infections involving all the premolar teeth.
Conclusion
Whether it is worth it to the GDP to invest the time and money required to invest in a Thermography Camera is an open question. It may be considered worthwhile in large group practices as an additional diagnostic aid especially if a lot of surgery is being done. Certainly for us the investment has been worthwhile. As a screening instrument it has told us which patients warrant further investigation without being detrimental in any way to the patient. As a diagnostic tool in specialist surgical environments it would be useful as well in diagnosis and monitory patients post operatively.
References
- Sukharev MF, Ivanova RP, Reitsman DM. Thermography in Inflammatory Odontogenic Processes. Stomatolgiia (Mosk) 56(4): 37-9. Jul-Aug 1977.
- Wesley E Shankland DDS . Osteocavitations of the Jaws. Townsend Newsletter 32(2). 2008.
- Lee H, Kim SG. Application of infrared thermography in dentistry. J Korean Assoc Oral Maxillofac Surg 31(4):335-341. Aug 2005.
- Dermot Dent Sc, MGDS, MS, Barton Grant DDS. Electronic thermography for the assessment of mild and moderate temperomandibular joint dysfunction. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology & Endodontology: 82(2): 145-151. Aug 1996.
- Valentim Adelino Ricardo Barão1), Ana Kelly Garcia Gallo1), Paulo Renato Junqueira Zuim1), Alicio Rosalino Garcia1) and Wirley Gonçalves Assunção. Effect of occlusal splint treatment on the temperature of different muscles in patients with TMD. Journal of Prosthodontic Research 55 (1): 19-23. 2011.
- Gamagami P. New Early Signs in Breast Cancer. Atlas of Mammography. Blackwell Press. 1996.
- Bernard Swerdlow, John Nathan I. Dieter. An evaluation of the sensitivity and specificity of medical thermography for the documentation of myofascial trigger points. Pain 48 (2): 205-213. February 1992.
Comments:
-
No Article Comments available