Positive Health Online
Your Country

![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Organic Aromatherapy]](/img/original/TopicbannerAvatar/1001.12a011c5d14492e86a5a2fa985244b74.jpg "Organic Aromatherapy")
![[Image: Lotus Books]](/img/original/TopicbannerAvatar/953.adb373b0210368e0c9ce4d9a8a9f01aa.jpg "Lotus Books")
![[Image: ICAN International Clinical Aromatherapy Network]](/img/original/TopicbannerAvatar/4442.566a83a07de79de73b9c738f7fb6458a.jpg "ICAN International Clinical Aromatherapy Network")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
![[Image: IFPA Int'l Fed Aromatherapists]](/img/original/TopicbannerAvatar/1185.9b7a831d484259621c55f48bd9933c3a.jpg "IFPA Int'l Fed Aromatherapists")
Bolles Sensory Learning Method
listed in learning difficulties, originally published in issue 62 - March 2001
Introduction
The Bolles Sensory Learning Method™ is an innovative non-cognitive approach to developmental learning that utilizes enhanced natural sensory stimulation for remediation of an individual's emergent faculties. The brain's ability to process and organize sensations of sight, sound and gravity begins to emerge in the womb and continues into adolescence. Sensory stimulation plays a major role in shaping the structure and functioning of the brain. The brain can be thought of as a sensory processing machine. So by stimulating the senses we can enhance emergent faculties – normal subconscious sensory functioning in the brainstem area.
This educational method is highly successful across a wide spectrum of populations because 'our brains are more alike than they are different.' It is a therapy that accelerates sensory integration and develops learning abilities for individuals with acquired brain injury, learning/behavioural problems, ADD/ADHD, developmental delays, autism and birth trauma.
This approach re-educates emergent faculties by stimulating the participant's sensory systems to learn or relearn subconscious reception, processing and integration skills. The beneficial outcomes of the Bolles Sensory Learning Method are long lasting and continue to accrue over time.
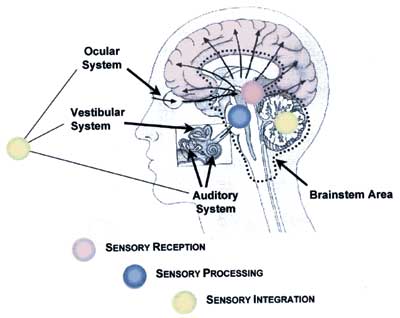
Sensory systems and their general location within the brain
The therapy modality uses key elements of three well-established sensory stimulation therapies combined into one simultaneous sensory experience. Combining the three modalities of photo stimulation, acoustic stimulation and vestibular stimulation has remarkably accelerated sensory integration and rehabilitation processes for participants.
A movement table delivering vestibular stimulation primes and unifies the nervous system arousing the brainstem area. When combined with coloured light frequencies and modulated sound frequencies, the computer-controlled instrumentation provides sessions that are at once kinaesthetic, integrative and desensitizing.
History
I grew up in rural Ohio and after earning a college degree in liberal arts I found my life almost totally focused on the learning and behavioural problems of the second of my four children. Born in the early 70s, he was not talking at three, he didn't seem to feel pain when he skinned his knee or hit his head, and his coordination didn't seem to be quite as good as that of other children when learning to swim. He seemed to lack any 'inner peace' and had difficulty with trust and bonding. He had anxieties and fears that were disproportionate to his experiences. When he stood in a line at school and a classmate bumped him he would begin striking out at the child. For him, the coming together of sensory input could not give reasonable meaning to his experience so he would become disoriented and act out feelings of anxiety, frustration and fear. Underactive sensory motor activity in his brainstem contributed to his hyperactivity and distractibility. This lack of sensory integration in my child became the focus of my life's work and led to the development of sensory learning.
Bolles sensory learning method
Over time I discovered that learning problems are much more that a reversal of letters, a language delay, hyperactive behaviour, or an attention deficit disorder. These problems involve all the dimensions in a child, and every child has its own individual mosaic which can be best addressed by a comprehensive approach. I learned that working with the whole to reach a child effectively and enhance his developmental potential requires us to engage the child fully. Therefore, I worked to create an experience that nurtured and challenged his subconscious sensory experience and could be engaging and fun on a conscious level. I became convinced that a therapy had to be delivered in a manner that felt supportive and safe so that the participant could maintain openness and receptivity. Medical interventions are so often 'done' to an individual while educational (learning) interventions are interactive in nature.
Sensory skills are learned through experiential interaction. I finally came up with three medical interventions that had been practised for over 40 years. The first of these was Dr Harry Riley Spitler who founded the college of Syntonic Optometry in 1933. As a pioneer in the field of photo stimulation he stated that 'syntony for balancing of the autonomic nervous system and the endocrine system can be produced by frequency of light in the eye'. The second, Dr Guy Berard, a French doctor who wrote Hearing Equals Behaviour, was a strong leader in the field of acoustic stimulation. He stated that 'everything happens as if human behaviour is largely conditioned by the manner in which one hears'. The third was Dr Jean Ayers, an occupational therapist. She formulated a theory of sensory integration dysfunction and developed interventions which included vestibular stimulation or bodily movement. She said, 'The vestibular system is the unifying system and vestibular stimulation seems to prime the whole nervous system to function more effectively.'
Development
More than ten years ago, I had an office in which I was doing the three modalities in separate rooms. Over time I learned that combining them into one simultaneous sensory experience provided a more natural, engaging, gentle and supportive therapy. Many professionals thought the idea was unsound because they believed it would be too overwhelming for the participant. I think the reason we saw overwhelm in the execution of the individual therapies was because we were isolating their deficited sensory system. With sensory learning, the deficited system is actually supported by the stronger, better functioning sensory systems.
For example, if a child demonstrated vision problems, working only with the modality involving visual stimulation was very difficult for the child and everyone else involved in the process. The child became totally overwhelmed and spent his energy resisting the therapy. The senses need to work interdependently as the conscious brain cannot make sense of sensory messages until they are integrated. Sensory messages come in as subconscious reflex transmissions. Messages about sound and motion enter by way of the cochlear-vestibular nerve into a very primitive area of the brainstem called the medulla oblongata. Ocular messages come into the brainstem to an area just above that called the pons. These messages must become integrated before they come into conscious awareness in the cortex. Without integration the conscious messages that are received are inaccurate and confusing. They give rise to frustration, anxiety and distractibility. They create perception problems such as not being able to think in sequence, not being able to understand verbal instructions or know where a sound is coming from. Some children are so gravitationally insecure that they have difficulty walking on uneven ground or are afraid to ride on a piece of playground equipment that moves. Others are so sensitive auditorially that they always act startled as if in pain from the noise of a blender or hairdryer in their home. Some children have difficulty reading because the words 'won't hold still on the page'. The successful integration of these messages gives rise to the emergence of sensory abilities or faculties we mostly take for granted because they occur largely subconsciously. For individuals with an acquired brain injury, activities that were once routine like reading become difficult, and previously comfortable environments like restaurants become auditorially stressful and overwhelming.
Principles
The sensory learning process is based on the principle of neuroplasticity. In part, this is the ability of the brain to reorganize itself continually throughout life from the sensory inputs it receives. Neuroscientific research in the 1990s shows that a brain older than three years is not a rigid structure, a belief long held by many scientists.
An underlying hypothesis of combining the frequencies of light, sound and motion into one sensory experience is that this combination is present in the womb. As early as nine weeks the foetus feels gravity and later senses movement or vestibular stimulation when the mother moves. Acoustic stimulation in the form of the mother's heartbeat and voice as well as sounds from the environment both arouse and pacify the developing foetus. The electromagnetic frequency of magenta provides photo stimulation of a vibrational nature in the womb experience. Understanding that the womb experience does shape the structure and functioning of the developing brain and nervous system, I believe that similar sensory stimulation can reorganize and reintegrate the brain.
Both mild and profound brain dysfunctions are primarily sensory in nature. Today there are many labels, such as autism, which are used for these different levels of dysfunction but they are all part of the same spectrum of sensory disorder. Well-modulated sensory motor activity in the brainstem area is instrumental in helping to maintain a calm, alert state. Ineffective and irregular subconscious sensory processing in the brainstem area results in hypersensitivity, sensory overwhelm, slowed ability to process information, speech impairment, memory loss, lack of concentration, and visual balance disorder. The child struggling with distractibility, hyperactivity, impulsivity and disorganization is often out of relationship with his environment because his emergent faculties are not fully developed.
Sensory learning is different from many therapeutic approaches because it works with the brain from the bottom up instead of from the top down. It is a non-cognitive approach and its effects take place below the conscious level, optimizing brainstem organization and integration. Tutoring and counselling, teaching coping skills, and doing cognitive retraining are attempting to work from the top down. Sensory Learning acknowledges physical functioning problems in the brainstem area and works from the bottom up to eliminate hypersensitivities, re-establish better timing and integration of sensory messages, and normalize neurological development. When sensory functioning is effortless and integrated, the individual is highly adaptive, body movements are well co-ordinated, learning is easy, and appropriate behavioural responses are natural outcomes. The therapy brings forth the ability to handle complex sensory activities and environments which were previously impossible and often overwhelming.
Sensory learning has always had varying degrees of positive responses but in some cases the full potential of improvement may be compromised because the individual or the family of the child is not willing to look at the need for biological treatments, detoxification, or dietary modification. The reverse is also true: boosting the immune system and improving digestion without a comprehensive sensory stimulation programme to enhance emergent faculties can limit the possibilities of partially or fully resolving many sensory problems.
Application
An integrated system utilizing high technology equipment, instruments and software was specifically developed for the application of sensory learning. It uses enhanced natural sensory stimulation consisting of an integrated, computer- controlled progression of sensory inputs that stimulate a highly focused interplay between the participant's three primary sensory systems.
Designed for individual application, the sensory learning process takes place in a completely darkened room. Lying on a moving table, the person receives gentle, precise patterns of circular movement. This vestibular stimulation circulates fluid in the semi-circular canals of the inner ear. When a baby is rocked, the motion calms and relaxes him. He trusts that he is safe, and this movement allows him to enter an altered state. As adults, a day of boating or a long train ride can give us a similar experience of repetitive rhythmic motion and the sense of a time when our nervous system was supported in a profoundly relaxed state.
In addition to this pleasant, engaging sensation of motion, the eyes are drawn to follow a coloured light positioned above the eyes. The stationary light provides an aerobic activity for the extrinsic eye muscles. The light progresses through six different frequencies (colours) as it is slowly dimming and brightening. At the same time, music, which is randomly attenuated at different frequencies, is being received through headphones.
With this much sensory input being presented one cannot armour against any of it individually, or be totally aware of all of it. The sensory input is unusual, unpredictable, and uniquely arousing. It challenges the general spatial/temporal orientation of the individual session after session.
Delivered over a 30-day period, the programme is 12 consecutive days of hour-long sessions followed by an 18-day home programme of photo stimulation alone.
The visual and auditory perception of the participant is assessed before and throughout the programme to determine computer settings and to monitor progress. Visually, we are evaluating photocurrent intake and measuring visual field constriction and expansion. Auditorially, we are measuring uneven listening ability, imprinted sensitivities and patterns, and then intervene with specific filtering and ear dominance techniques to promote and establish more even listening abilities.
Case Summaries
Case Summary 1
A 4-year-old girl diagnosed with autism.
Background – Foetal distress at birth. Evaluated at 23 months. Problems with language development, social relatedness, difficult behaviour and unusual habits like walking in circles. Frequent temper tantrums and head banging. Gravitationally insecure.
Presenting Symptoms – Poor eye contact and unable to be present with the social environment of the moment (in her own withdrawn world). Fairly antisocial, easily upset, lacking in spontaneous language, sensory integration problems, slightly behind in gross and fine motor skills, difficult to motivate.
Realized Outcomes – During the first 30 days, she began to come present with the social environment of the moment: began to say her own name repeatedly; noticing things she never noticed before and began responding to communication directed specifically to her. Eye contact improved.
One year after the sensory learning intervention, the evaluating doctor noted remarkable progress from the autistic symptoms. The mother wrote that 'the doctor said that she was the highest functioning autistic child she had ever seen, and she thinks we should send her to kindergarten with no label, no diagnosis and no individual educational programme to see how it goes!' The evaluating doctor summarized the second year's annual review as follows: 'In this sample of her behaviour, she did not demonstrate symptoms of an autistic spectrum disorder, or of any other disorder.'
Case Summary 2
A 39-year-old male executive.
Background – Mild traumatic brain injury resulting from motor vehicle accident 18 months prior to completing sensory learning.
Presenting Symptoms – Could not hold a thought, finish a sentence, have any type of multiple input or even listen to a radio. Speech was deliberate and always searching for words. Frequent feelings of panic and depression. Frequently experienced run-away thoughts. Only able to work at one-tenth capacity and only during off-hours when quiet. Difficulty sorting mail.
Realized Outcomes – Within the first few sessions he experienced improvement: able to listen to the radio; once again able to tell a joke and remember the punch line; regained ability mentally to calculate a tip; no longer overwhelmed by noisy social situations such as restaurant conversations; returned to normal work hours and output.
Case Summary 3
A 6-year-old girl with learning and behaviour problems.
Participant unable to follow directions for evaluation.
Background – Foetal distress late in pregnancy due to the cord around the neck seven times; emergency c-section delivery. Incurred a fall onto some bricks at 41/2 years requiring dental and gum surgery. Severe behaviour problems, learning problems, and social problems resulted in a difficult first school year.
Presenting Problems – She seemed to be always angry and explosive. She didn't express herself well with language. She was always saying: "I don't understand". The teachers at school were not looking forward to having to deal with her the next year. She had no friends.
Realized Outcomes – During the first 30 days, it appeared to the mother that the intervention intensified her reactive personality and her uncooperative nature. At the end of the 12 days the mother felt there had been no improvement.
It was weeks later that the mother and other caregivers began to see positive changes in her behaviour. Overall, she became calmer, softer, less explosive. In situations where she used to get angry, she was less reactive. The mother said, "I'm so glad we're beginning to get this unwound". Mother reported that her language and auditory processing were much improved.
At 3-6 months following the intervention, definite, solid improvement could be seen in her learning abilities, her behaviour and social skills at school. The family did no other therapies with the child during this time and feel sensory learning 'turned the child around 180 degrees'. Many of the teachers asked what the mother did with the child over the summer to bring about the dramatic changes they observed.
Case Summary 4
A 7-year-old boy with learning problems.
Background – History of dyslexia on both sides of the family; attended a private school which specialized in children with learning problems; it was determined that he had visual processing problems.
Presenting Problems – He was confused by letters, numbers, words, sequences and verbal explanations. He seemed to 'zone out' or daydream often. He had difficulty sustaining attention and seemed 'hyper'.
Realized Outcomes – During the first 30 days, his mother noted that he was a much more 'settled' child than before the sessions; he seemed to lose his fear of letters and words and began to make progress with his reading which improved noticeably.
One year later, the child was able to transfer from the private school to a public school. As a result of his improvements, his younger brother and father both completed sensory learning.
Case Summary 5
A 4-year-old girl with learning and behaviour problems.
Background – Adopted as an infant; foetal alcohol syndrome.
Presenting Problems – Almost no attention span, poor sequential memory; difficulty putting thoughts into words – speaks in halting phrases; severe difficulty with word retrieval, even naming foods she eats almost every day; difficulty interacting with other children.
Realized Outcomes – She quit wetting her pants in the day. She has better eye contact and less oppositional behaviour. Mother reports good interaction on playground with young friends. There is marked improvement in verbalizing recent events in proper sequence. She no longer asks the same questions over and over as if she hasn't heard the explanations given. Mother reports speech development has evolved beautifully. She is doing well in school with no major behaviour problems.
Comments:
-
No Article Comments available