Positive Health Online
Your Country

![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Organic Aromatherapy]](/img/original/TopicbannerAvatar/1001.12a011c5d14492e86a5a2fa985244b74.jpg "Organic Aromatherapy")
![[Image: Human Kinetics Trail Guide to the Body]](/img/original/TopicbannerAvatar/4656.d9ccc329faa3d1500b4807b369feccef.jpg "Human Kinetics Trail Guide to the Body")
![[Image: Lotus Books]](/img/original/TopicbannerAvatar/953.adb373b0210368e0c9ce4d9a8a9f01aa.jpg "Lotus Books")
![[Image: ICAN International Clinical Aromatherapy Network]](/img/original/TopicbannerAvatar/4442.566a83a07de79de73b9c738f7fb6458a.jpg "ICAN International Clinical Aromatherapy Network")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
![[Image: SG Cancer Book]](/img/original/TopicbannerAvatar/960.4f24bbd158abe4427cc06911969143e5.jpg "SG Cancer Book")
Letters to the Editor Issue 270
listed in letters to the editor, originally published in issue 270 - May 2021
Singapore Scientists Develop Diagnostic Test to Detect the COVID-19 Virus
A team of scientists led by Nanyang Technological University, Singapore (NTU Singapore) has developed a diagnostic test that can detect SARS-CoV-2 – the virus that causes COVID-19 – even after it has gone through mutations. Called the VaNGuard (Variant Nucleotide Guard) test, it makes use of a gene-editing tool known as CRISPR, which is used widely in scientific research to alter DNA sequences and modify gene function in human cells under lab conditions, and more recently, in diagnostic applications. Since viruses have the ability to evolve over time, a diagnostic test robust against potential mutations is a crucial tool for tracking and fighting the pandemic. Over its course so far, thousands of variants of SARS-CoV-2, the virus that causes COVID-19, have arisen, including some that have spread widely in the United Kingdom, South Africa, and Brazil[1].
However, the genetic sequence variations in new strains may impede the ability of some diagnostic tests to detect the virus, said NTU Associate Professor Tan Meng How, whose team includes researchers from the National University Health System and the Agency for Science, Technology and Research, Singapore (A*STAR). In addition to its ability to detect SARS-CoV-2 even when it mutates, the VaNGuard test can be used on crude patient samples in a clinical setting without the need for RNA purification, and yields results in 30 minutes. This is a third of the time required for the gold standard polymerase chain reaction (PCR) test, which requires purification of RNA in a lab facility.
The team of scientists led by NTU hopes that the VaNGuard test can be deployed in settings where quickly confirming COVID-19 status of individuals is paramount. Associate Professor Tan, who is from NTU’s School of Chemical and Biomedical Engineering, said:
“Viruses are very smart. They can mutate, edit, or shuffle their genetic material, meaning diagnostic tests may fail to catch them. Hence, we spent considerable effort developing a robust and sensitive test that can catch the viruses even when they change their genetic sequences. In addition, frequent testing is essential for helping to break the transmission of viruses within populations, so we have developed our tests to be rapid and affordable, making them deployable in resource-poor settings.”
The findings were published in scientific journal Nature Communications on 19 March.[2]
The research team has filed a patent for the VaNGuard test. Moving forward, they plan to perform further experiments to further refine their diagnostic kit, obtain regulatory approval from relevant authorities, and commercialise their test in partnership with diagnostic companies.
Using a Pair of “Molecular Scissors” to Detect Virus
The VaNGuard test relies on a reaction mix containing enAsCas12a, a variant of the enzyme Cas12a that acts like a pair of “molecular scissors”.
The enzyme enAsCas12a is ‘programmed’ to target specific segments of the SARS-CoV-2 genetic material and to snip them off from the rest of its viral genome. Successfully snipping off segments is how the enzyme ‘detects’ the presence of the virus. The programming is done by two different molecules known as guide RNAs, which are designed to recognize specific sites on the SARS-CoV-2 genome. The scientists decided to use two guide RNAs that recognise sequences that are extremely similar between variants of SARS-CoV-2 and that are also unique to the virus. Each guide RNA is computationally predicted to recognize over 99.5 per cent of the thousands of SARS-CoV-2 isolates that have so far been sequenced around the world.
Assoc. Prof Tan explained:
“Combining two or more guide RNAs with the enzyme enAsCas12a ensures that if one of the guide RNAs fails to guide it to the correct segment of the virus because of a mutation, the other guide RNA can still ‘rescue’ this mismatch.”
So far, the made-in-NTU diagnostic platform can recognize up to two mutations within the target sites on the SARS-CoV-2 genome. When the SARS-CoV-2 virus or one of its variants is detected in a sample, the engineered Cas12 enzyme variant enAsCas12a becomes hyper-activated and starts cutting other detectable genetic material in the sample as well, including a molecule tagged with a fluorescent dye that is added to the reaction mix.
When the molecule is cut, it starts to glow. This glow is picked up by a microplate reader, a lab instrument that can detect and quantify the light photons emitted by the molecule.
Assoc. Prof Tan, who is also from the Genome Institute of Singapore at A*STAR, explained:
“If the virus is present, the molecule will glow. If not, it means the virus is not present to cause the hyper-activation of the molecular scissors.”
Making the VaNGuard Test Easy to Use
To make the test easier to use once it has been approved for roll out, the scientists integrated the test into a specially treated paper strip that looks similar to a pregnancy test. The paper strip is dipped into a tube containing the crude nasopharyngeal sample and the reaction mix. In the presence of a SARS-CoV-2 virus or its variant, two strong bands will appear on the paper strip. In the absence of the virus, only one band will appear.
The scientists validated the VaNGuard test’s ability to detect SARS-CoV-2 variants by synthesizing an RNA sample that has the same mutated sequence as a known SARS-CoV-2 variant. They added different amounts of the synthesised sample to their test and observed two strong bands when the paper strip was dipped into each reaction mix. This indicates that the VaNGuard test is robust against mutated viral sequences. The scientists also developed a mobile phone app to facilitate the interpretation of the paper strips. The VaNGuard test was developed by scientists from NTU’s School of Chemical and Biomedical Engineering, School of Biological Sciences, and School of Computer Science and Engineering; National University Health System; and A*STAR.
About Nanyang Technological University, Singapore
A research-intensive public university, Nanyang Technological University, Singapore (NTU Singapore) has 33,000 undergraduate and postgraduate students in the Engineering, Business, Science, Humanities, Arts, & Social Sciences, and Graduate colleges. It also has a medical school, the Lee Kong Chian School of Medicine, established jointly with Imperial College London. NTU is also home to world-class autonomous institutes – the National Institute of Education, S Rajaratnam School of International Studies, Earth Observatory of Singapore, and Singapore Centre for Environmental Life Sciences Engineering – and various leading research centres such as the Nanyang Environment & Water Research Institute (NEWRI) and Energy Research Institute @ NTU (ERI@N). Ranked amongst the world’s top universities by QS, NTU has also been named the world’s top young university for the past seven years. For more information, visit www.ntu.edu.sg .
References
- ‘About variants of the virus that causes COVID-19’, Centers for Disease Control and Prevention. https://www.cdc.gov/coronavirus/2019-ncov/transmission/variant.html
- Kean Hean Ooi et al. An engineered CRISPR-Cas12a variant and DNA-RNA hybrid guides2 enable robust and rapid COVID-19 testing. Nature Communications: 12: 1739. 2021. DOI: 10.1038/s41467-021-21996-6
Further Information
Foo Jie Ying <jieying@ntu.edu.sg>
Manager, Corporate Communications Office, Nanyang Technological University
Rutherford Health Announces Expansion of Proton Therapy Training for Oncologists
Rutherford Health, the UK and Europe’s leading provider of proton beam therapy services, has announced that its proton training programme for oncologists has been expanded to meet rising demand. The course was designed in collaboration with the University of Pennsylvania and IBA Worldwide, the largest manufacturer of proton therapy machines, and gives oncologists certification to administer high energy proton beam therapy in cancer patients.
Rutherford Health created the training programme 3 years ago and over 35 oncologists have become certified in proton beam therapy. A further 20 oncologists have been enrolled onto the programme over the next two months alone. Rutherford’s centres offer proton beam therapy to insured, self-pay and NHS patients where they have been Commissioned to offer a service and demand has been soaring.
The two-part programme involves an e-learning module called Oncolink delivered by IBA Worldwide followed by a course with the University of Pennsylvania which is currently done virtually due to the pandemic. The course takes 2 weeks to complete depending on the flexibility of trainee oncologists.
Professor Karol Sikora, Medical Director of Rutherford Cancer Centres, said:
“The growth of our proton therapy programme is another hugely encouraging sign that advanced cancer care continues to move forward with wider adoption of treatments which can improve health outcomes.
“The training programme has attracted oncologists working in the NHS who will be able to widen access and provision to advanced treatments such as proton beam therapy for their patients and improve the overall quality of cancer care.
“Until proton therapy became available in the UK, the number of oncologists trained in the delivery of this treatment was understandably limited. The growth in training reflects the increasing awareness of proton beam therapy as a treatment option. Certainly in the insured and self-pay market we have seen increasing demand for proton beam therapy as patients seek advanced treatments which can reduce side effects and maintain a good quality of life.
“The rise in demand for the programme in recent months is due to a number of factors including the urgency of the cancer backlog and the widespread adoption of proton beam therapy in the UK. Personnel training is crucial in order to keep up with the latest advances in cancer treatments and programmes such as ours will ensure the UK has the necessary talent and skill to incorporate the most advanced treatment for cancer for years to come.”
Rutherford Health operates a network of three proton beam therapy centres, with a fourth centre due to start offering proton beam therapy next year. It is the largest integrated network of proton therapy facilities in the world. The centre in Wales was the first to bring the treatment to the UK in 2018. In addition to the Rutherford, the NHS also operates a proton facility at the Christie NHS Foundation Trust in Manchester with a second NHS facility still under construction at UCLH in Central London.
Source and Further Information
For further information please contact Ramsay Smith (ramsay@mediahouse.co.uk) or Ibrahim Khalil (ibrahim@mediahouse.co.uk): Ibrahim: 07943 759 042; Ramsay: 0788 414 856.
About Rutherford Health plc
Rutherford Health plc offers a comprehensive range of the latest technology in cancer treatments, and is the only independent provider of proton beam therapy ("PBT") in the UK. The Company also provides conventional radiotherapy, chemotherapy, immunotherapy, imaging and wellbeing services. For more information, visit the Group's website: www.rutherfordhealth.com .
The VICTAS Trial: Designed to Fail
by Michael Passwater
Published from: orthomolecular.activehosted.com
A recent clinical research article concludes, "Among critically ill patients with sepsis, treatment with vitamin C, thiamine, and hydrocortisone, compared with placebo, did not significantly increase ventilator- and vasopressor-free days within 30 days. However, the trial was terminated early for administrative reasons and may have been underpowered to detect a clinically important difference." [1] For some medical professionals, that study is proof that "HAT Therapy" (Hydrocortisone, Ascorbic acid, Thiamine), and vitamin C is not helpful in the treatment of sepsis. But such a conclusion is a dangerous over-generalization of the study's findings.
Rather than focus on the early termination of the study, a more concerning aspect is its design. The treatment for the subjects included in the analysis was not required to begin quickly. The study treatments were given many hours (median 14.7) after subjects' sepsis symptoms worsened into cardiovascular or respiratory failure. The intravenous (IV) vitamin C dose was limited and fixed at 1.5g every 6 hours (86 mg/kg/day; 6g per day for a 70 kg subject), and the duration of treatment was limited to 4 days. The protocol did not require measurements of vitamin C, thiamine, or cortisol in study subjects before, during, or after treatment, and no measurements were reported in the article. Further, no measures of other co-nutrients were included. For instance, a low vitamin D level is an established biomarker of all-cause mortality in the ICU setting. [2] Low zinc, magnesium, and selenoprotein levels, as well as anaemia, have also been associated with poor outcomes in critical care, including viral sepsis. [3-8] The article does not say whether the treatment and control groups were balanced at study entry with respect to vitamin C and other nutrient levels, nor whether adequate vitamin C was given to maintain plasma levels in the therapeutic range during the study. The "Limitations" section of the article acknowledges "...a higher dose or dosing based on plasma vitamin C concentrations might yield different results."
In both the Test and Control arms of the study, the per protocol mortality before ICU discharge was 16.6% and 17.0% respectively (p=0.91), and at 180 days was 39.5% and 36.8% respectively (p=0.57). Neither standard treatment nor the delayed addition of low dose IVC for a short duration improved the poor survival of sepsis in this study. The overall conclusion that one can draw from this VICTAS trial is that vitamin C is safe, but that too little, too late, for too short of a duration is inadequate.
50 years ago, Dr Frederick R. Klenner published a summary of his experience and prior publications. [9] He encouraged a daily IV dose of 350 - 700 mg vitamin C per kg of patient body weight (25,000 - 50,000 mg for a 70 kg / 154 lb subject), increasing the dose and frequency as necessary until the patient recovered:
"It is a demonstrated principle that the production of histamine and other end products from deaminized cell proteins released by injury to cells are a cause of shock. The clinical value of ascorbic acid in combating shock is explained when we realize that the deaminizing enzymes from the damaged cells are inhibited by vitamin C. It has been shown by Chambers and Pollock [10] that mechanical damage to a cell results in pH changes which reverse the cell enzymes from constructive to destructive activity. The pH changes spread to other cells. This destructive activity releases histamine, a major shock producing substance. The presence of vitamin C inhibits this enzyme transition into the destructive phase. Clark and Rossiter [11] reported that conditions of shock and stress cause depletion of the ascorbic acid content of the plasma. As with the virus bodies, ascorbic acid also joins with the protein factor of these toxins effecting quick destruction. The answer to these emergencies is simple. Large amounts of ascorbic acid 350 mg to 700 mg per kg body weight given intravenously. In small patients, where veins are at a premium, ascorbic acid can easily be given intramuscularly in amounts up to two grams at one site. Several areas can be used with each dose given. Ice held to the gluteal muscles until red, almost eliminates the pain. We always reapply the ice for a few minutes after the injection. Ascorbic acid is also given, by mouth, as follow-up treatment. Every emergency room should be stocked with vitamin C ampoules of sufficient strength so that time will never be counted as a factor in saving a life. The 4 gram, 20 cc ampoule and 10 gram 50 cc ampoule must be made available to the physician."
The CITRIS-ALI study used 50 mg vitamin C per kg patient weight per treatment (200 mg/kg/day; 14g per day for a 70 kg subject) - more than double the dose used in the VICTAS Trial - yet less than one third of the upper range promoted by Dr Klenner. Moreover, the CITRIS-ALI study showed a clear survival benefit (mortality was a secondary endpoint in that trial). [12] This dose of 200 mg/kg/day was also used by the earlier Phase I safety trial of IVC in sepsis. [13]
Why, years later, did the VICTAS Trial choose to use less than half that dose? What would happen if a trial was done using efficacious doses – those shown for over 70 years to help real people recover from critical illness? Doctors who utilize this protocol don't go back to treating patients without it.
In the January 20, 2021 OMNS article "The Treatment of Infectious Disease Using Vitamin C and Other Nutrients" Margot DesBois nicely covers the early history of IVC use in serious illness. [14] In addition to Drs. Frederick Klenner, Claus Jungeblut, Robert Cathcart, and William McCormick, more recent clinical medicine pioneers including Drs. Hugh Riordan, Ron Hunningshake, AA Fowler, Paul Marik, and Joseph Varon can be added to the list. [15-21]
Of note, the most successful published protocol for Covid-19 hospital treatment in the USA includes 3g IVC per dose along with a corticosteroid and thiamine every 6 hours, and the use of 25g IVC doses if rescue therapy is needed. And the treatments are not stopped at 96 hours. The idea that giving vitamin C beyond 96 hours might be dangerous has no scientific or clinical basis. See the full COVID-19 treatment plan, [22] and the Riordan Clinic IVC protocol. [23]
As a reminder for those conducting and reviewing nutrient research, here are "rules" published by vitamin researcher Robert P. Heaney. [24]
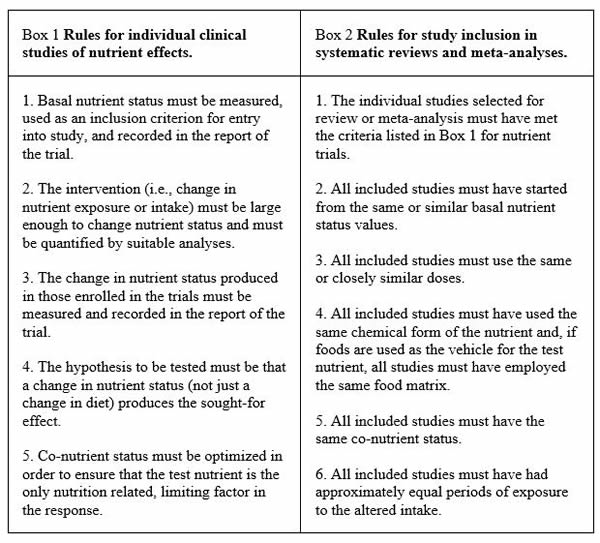
The VICTAS Trial [1] satisfied none of these 5 rules for conducting nutrient research.
Recent research has shown the importance of vitamin C in sepsis and other acute life-threatening illnesses. Vitamin C has a multitude of essential for life effects within the human body, and due to its short half-life, is often the rate limiting factor in these biochemical processes. It is the primary extracellular antioxidant, and is important for scavenging damaging electron radicals. At very high levels it is involved in redox regulation, is a pro-oxidant, and can cause DNA and/or protein damage. This is useful in the treatment of cancer. It is an essential co-factor in the synthesis of catecholamines, vasopressin, steroids, neuropeptides and some neurotransmitters. It is also essential in the synthesis of collagen and elastin -- which are important molecules throughout the body, including in arteries and joints. Vitamin C is also important for epigenomic regulation of genes and is necessary for many cell types of the adaptive immune system. These biochemical functions are essential for improved immune cell function, endothelial cell function, hemodynamics (circulatory function), and wound healing.
Stress, including cold temperatures, toxins, infections, and trauma greatly increase the cellular demand for vitamin C, and disrupt the body's ability to recycle oxidized vitamin C (dehydroascorbic acid or DHAA) back into the reduced form of vitamin C (ascorbic acid). Vitamin C has a short half-life in the body (minutes to hours). In 2008, the prestigious journal Cell published the discovery that the red blood cells of humans (and other mammals unable to produce vitamin C) express a large number of GLUT1 transporters – more GLUT1 than on any other human cell type. [25] These GLUT1 transporters are apparently misnamed, as they might more properly be called DHAA1 transporters. The human RBC GLUT1 transporter is co-expressed with the protein stomatin which switches it into a DHAA transporter rather than a glucose transporter. [25] The result is 20-30 trillion red blood cells in healthy humans circulating through miles of blood vessels "soaking up" DHAA and – if adequate levels of the selenoprotein glutathione peroxidase are present in the red blood cells – reducing the DHAA back to AA and sending it back into the blood. A similar recycling system is present in the brain between astrocytes and tanycytes. [26] This supports the concept that keeping the blood, vasculature, and brain bathed inadequate ascorbic acid is important.
Humans in acute distress from toxins, viruses, and bacteria have been successfully treated with high dose vitamin C injections for over 70 years. Recent studies have shown a synergistic benefit to endothelial cells when vitamin C and cortisol are injected into blood vessels simultaneously. Decades of experience have underscored the importance of early intervention, and increasing the dose and duration as needed to neutralize the acidosis and/or toxins. [27-53]
Below is a graph courtesy of Dr Paul E Marik of an ICU patient's c-reactive protein level (biomarker of inflammation) during 3g IVC and a corticosteroid co-administration every 6 hours for 96 hours, stopping the treatment, and then resuming the treatment. Continued vitamin C treatment until full recovery, tapering from IV to oral administration as the patient recovers, is important. It takes ongoing administration of vitamin C to achieve and maintain the tissue saturation levels needed to treat sepsis and septic shock.
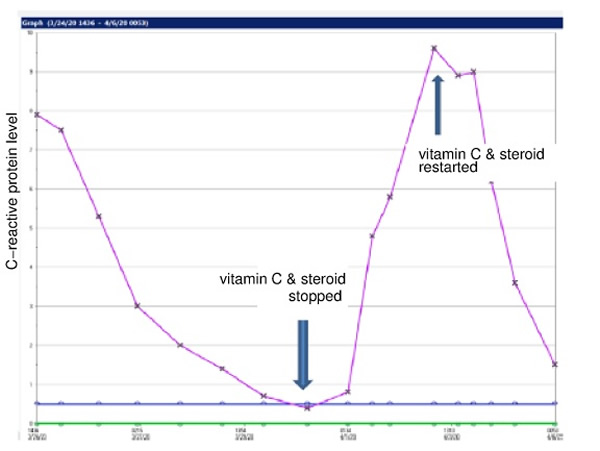
An ICU patient's c-reactive protein level (biomarker of inflammation) during 3g IVC and a corticosteroid co-administration every 6 hours for 96 hours, stopping the treatment, and then resuming the treatment
Is 70 years of successful treatments to thousands of patients insufficient evidence? If more studies are needed, who will put the 350-700 mg/kg/day IVC dose to the test without the dangerous and artificial 96-hour limitation?
Acknowledgements
I would like to acknowledge Benjamin Rakotoambinina MD PhD Professor of Physiology at the University of Antananarivo, Madagascar in collaboration with Laurent Hiffler MD of the Cellular Nutrition Research Group for their critical review and feedback; and Drs Robert G. Smith and Andrew Saul for their critical review and editorial support.
About the Author
Michael E Passwater, son of author and columnist Dr Richard Passwater, is certified by the American Society for Clinical Pathology as a medical technologist, a specialist in immunohematology, and is a diplomate in laboratory management. He has worked in clinical laboratories for 28 years, and has previously written “Do the Math: "MATH+" Saves Lives” published by the Orthomolecular Medicine News Service http://orthomolecular.org/resources/omns/v16n55.shtml .
References
- Sevransky JE, Rothman RE, Hager DN, et al. (2021) Effect of Vitamin C, Thiamine, and Hydrocortisone on Ventilator-and Vasopressor-Free Days in Patients With Sepsis: The VICTAS Randomized Clinical Trial. JAMA 325:742-751. https://jamanetwork.com/journals/jama/fullarticle/2776688
- Moraes RB, Friedman G, Wawrzeniak IC, et al. (2015) Vitamin D deficiency is independently associated with mortality among critically ill patients. Clinics. 70:326-332. https://pubmed.ncbi.nlm.nih.gov/26039948
- Alker W, Haase H. (2018) Zinc and Sepsis Nutrients 10:976. https://pubmed.ncbi.nlm.nih.gov/30060473
- Noormandi A, Khalili H, Mohammadi M, et al. (2020) Effect of magnesium supplementation on lactate clearance in critically ill patients with severe sepsis: a randomized clinical trial. Eur J Clin Pharmacol 76:175-184. https://pubmed.ncbi.nlm.nih.gov/31814044
- Velissaris D, Karamouzos V, Pierrakos C, et al. (2015) Hypomagnesemia in critically ill sepsis patients. J Clin Med Res 2015;7:911-918. https://pubmed.ncbi.nlm.nih.gov/26566403
- Guerin C, Cousin C, Mignot F, et al. (1996) Serum and erythrocyte magnesium in critically ill patients. Intensive Care Med 22:724-727. https://pubmed.ncbi.nlm.nih.gov/8880238
- Angstwurm MW, Engelmann L, Zimmermann T, et al. (2007) "Selenium in Intensive Care (SIC): results of a prospective randomized, placebo-controlled, multiple-center study in patients with severe systemic inflammatory response syndrome, sepsis, and septic shock." Crit Care Med. 35:118-26. https://pubmed.ncbi.nlm.nih.gov/17095947
- Belsky JB, Wira CR, Jacob V, et al. (2018) A review of micronutrients in sepsis: the role of thiamine, l-carnitine, vitamin C, selenium and vitamin D. Nutr Res Rev. 31:281-290. https://pubmed.ncbi.nlm.nih.gov/29984680
- Klenner FR. (1971) Observations On the Dose and Administration of Ascorbic Acid When Employed Beyond the Range of A Vitamin In Human Pathology. J Applied Nutrit. 23:61-87. https://seanet.com/~alexs/ascorbate/197x/klenner-fr-j_appl_nutr-1971-v23-n3&4-p61.htm
- Chambers R, Pollock H. (1927) Micrurgical studies in cell physiology: IV. Colorimetric determination of the nuclear and cytoplasmic pH in th e starfish egg. J Gen. Physiol 10:739-755. https://pubmed.ncbi.nlm.nih.gov/19872358/
- Clark EJ, Rossiter RJ. (1944) Carbohydrate metabolism after burning. Q J Exp Physiol Cog Med Sci 32:279-300. https://doi.org/10.1113/expphysiol.1944.sp000890
- Fowler AA, Truwit JD, Hite RD, et al. (2019) Effect of Vitamin C Infusion on Organ Failure and Biomarkers of Inflammation and Vascular Injury in Patients With Sepsis and Severe Acute Respiratory Failure: The CITRIS-ALI Randomized Clinical Trial. JAMA 322:1261-1270. https://pubmed.ncbi.nlm.nih.gov/31573637
- Fowler AA, Syed AA, Knowlson S, et al. (2014) "Phase I Safety trial of intravenous ascorbic acid in patients with severe sepsis." J Transl Med 12:32. https://pubmed.ncbi.nlm.nih.gov/24484547
- DesBois M (2021) The Treatment of Infectious Disease Using Vitamin C and other Nutrients. Orthomolecular Medicine News Service. http://orthomolecular.org/resources/omns/v17n04.shtml
- Klenner FR (1949) The Treatment of Poliomyelitis and other Virus Diseases with Vitamin C. South Med Surg. 111:209-214. https://pubmed.ncbi.nlm.nih.gov/18147027 https://vitamincfoundation.org/www.orthomed.com/polio.htm https://www.seanet.com/~alexs/ascorbate/194x/klenner-fr-southern_med_surg-1948-v110-n2-p36.htm
- Jungeblut CW (1935) Inactivation of Poliomyelitis virus in vitro by crystalline vitamin C (ascorbic acid) J Exp Med. 62:517-521. https://pubmed.ncbi.nlm.nih.gov/19870431
- Cathcart RF (1981) Vitamin C, titrating to bowel tolerance, anascorbemia, and acute induced scurvy. Med Hypotheses 7:1359-1376. https://pubmed.ncbi.nlm.nih.gov/7321921
- McCormick WJ (1951) Vitamin C in the Prophylaxis and Therapy of Infectious Diseases. Arch Pediatr. 68:1-9. https://pubmed.ncbi.nlm.nih.gov/14800557 https://www.seanet.com/~alexs/ascorbate/195x/mccormick-wj-arch_pediatrics-1951-v68-n1-p1.htm
- Hugh D Riordan HD, Hunninghake RB, Riordan NH, et al. (2003) Intravenous ascorbic acid: protocol for its application and use. P R Health Sci J, 22:287-90. https://pubmed.ncbi.nlm.nih.gov/14619456
- Marik PE, Khangoora V, Rivera R, Hooper MH, Catravas J. (2017) Hydrocortisone, Vitamin C, and Thiamine for the Treatment of Severe Sepsis and Septic Shock: A Retrospective Before-After Study. Chest 151:1229-1238. https://pubmed.ncbi.nlm.nih.gov/27940189
- Kory P, Meduri GU, Iglesias J, et al. (2021) Clinical and Scientific Rationale for the "MATH+" Hospital Treatment Protocol for COVID-19. J Intensive Care Med. 36:135-156. https://pubmed.ncbi.nlm.nih.gov/33317385
- Front Line COVID-19 Critical Care Alliance (2021) EVMS COVID-19 Management Protocol: An overview of the MATH+ and I-MASK+ Protocols. http://www.flccc.net
- Riordan H, Riordan, N, Casciari J (2021) The Riordan intravenous vitamin C (IVC) protocol for adjunctive cancer care: IVC as a chemotherapeutic and biologic response modifying agent. Riordan Clinic. https://riordanclinic.org/wp-content/uploads/2015/11/RiordanIVCprotocol_en.pdf
- Heaney RP. (2014) Guidelines for optimizing design and analysis of clinical studies of nutrient effects. Nutr Rev 72:48-54. https://pubmed.ncbi.nlm.nih.gov/24330136
- Montel-Hagen A, Kinet S, Manel N, et al. (2008) Erythrocyte Glut1 triggers dehydroascorbic acid uptake in mammals unable to synthesize vitamin C. Cell, 132:1039-1048. https://pubmed.ncbi.nlm.nih.gov/18358815
- Nualart F, Mack L, GarcÃa A, et al. (2014) Vitamin C Transporters, Recycling and the Bystander Effect in the Nervous System: SVCT2 versus Gluts. J Stem Cell Res Ther 4:209. https://pubmed.ncbi.nlm.nih.gov/25110615
- May JM, Harrison FE. (2013) Role of Vitamin C in the Function of the Vascular Endothelium. Antioxidants & Redox Signaling 19:2068-2083. https://pubmed.ncbi.nlm.nih.gov/23581713
- Nabzdyk CS, Bittner EA. (2018) Vitamin C in the critically ill - indications and controversies. World J Crit Care Med 7:52-61. https://www.wjgnet.com/2220-3141/full/v7/i5/52.htm
- Lee RE. (1961) Ascorbic Acid and the Peripheral Vascular System. Ann NY Acad Sci. 92:295-301. https://doi.org/10.1111/j.1749-6632.1961.tb46129.x
- Lee RE, Holze EA. (1951) Nutritional factors in hemodynamics: dissociation of pressor response and hemorrhage resistance in avitaminosis C. Proc. Soc. Expt. Biol Med. 76:325-329. https://pubmed.ncbi.nlm.nih.gov/14827915
- Barabutis N, Khangoora V, Marik PE, Catravas JD. (2017) Hydrocortisone and Ascorbic Acid Synergistically Prevent and Repair Lipopolysaccharide-Induced Pulmonary Endothelial Barrier Dysfunction. Chest 152:954-962. https://pubmed.ncbi.nlm.nih.gov/28739448
- Parker WH, Rhea EM, Qu ZC. (2016) Intracellular ascorbate tightens the endothelial permeability barrier through Epac1 and the tubulin cytoskeleton. Am J Physiol Cell Physiol. 311:C652-C662. https://pubmed.ncbi.nlm.nih.gov/27605450
- Gu W, Cheng A, Barnes H, et al. (2014) Vitamin C Deficiency Leading to Hemodynamically Significant Bleeding. JSM Clinical Case Reports 2:1046. https://www.jscimedcentral.com/CaseReports/casereports-2-1046.pdf
- Zhao B, Fei J, Chen Y, et al. (2014) Vitamin C treatment attenuates hemorrhagic shock related multi-organ injuries through the induction of heme oxygenase-1. BMC Complementary and Alternative Medicine 14:442-454. https://pubmed.ncbi.nlm.nih.gov/25387896
- Ladumer A, Schmitt CA, Schachner D, et al. (2012) Ascorbate stimulates endothelial nitric oxide synthase enzyme activity by rapid modulation of its phosphorylation status. Free Radic Biol Med. 52:2082-2090. https://pubmed.ncbi.nlm.nih.gov/22542797
- Heller R, Munscher-Paulig F, Grabner R, Till V. (1999) L-Ascorbic Acid Potentiates Nitric Oxide Synthesis in Endothelial Cells. J Biol Chem 274:8254-8260. https://pubmed.ncbi.nlm.nih.gov/10075731
- Dingchao H, Zhduan Q, Xiaodong F. (1994) The Protective Effects of High-Dose Ascorbic Acid on Myocardium against Reperfusion Injury During and After Cardiopulmonary Bypass. Thorac Cardiovasc Surg 42:276-278. https://pubmed.ncbi.nlm.nih.gov/7863489
- Ichim TE, Minev B, Braciak T, et al. (2011) Intravenous ascorbic acid to prevent and treat cancer-associated sepsis? J Transl Med 9:25. https://pubmed.ncbi.nlm.nih.gov/21375761
- Cisternas P, Silva-Alvarez C, Martinez F, et al. (2014) The oxidized form of vitamin C, dehydroascorbic acid, regulates neuronal energy metabolism. J Neurochem 129: 663-671. https://pubmed.ncbi.nlm.nih.gov/24460956
- Wang Y, Lin H, Lin BW, et al. (2019) Effects of different ascorbic acid doses on the mortality of critically ill patients: a meta-analysis. Ann Intensive Care 9:58. https://pubmed.ncbi.nlm.nih.gov/31111241
- Boretti A, Banik BK. (2020) Intravenous vitamin C for reduction of cytokines storm in acute respiratory distress syndrome. PharmaNutrition 12:100190. https://pubmed.ncbi.nlm.nih.gov/32322486
- Iglesias J, Vassallo AV, Patel V et al. (2020) Outcomes of metabolic resuscitation using ascorbic acid, thiamine, and glucocorticoids in the early treatment of sepsis. Chest 158:164-173. https://pubmed.ncbi.nlm.nih.gov/32194058
- de Melo AF, Homem-de-Mello M. (2020) High-dose intravenous vitamin C may help in cytokine storm in severe SARS-CoV-2 infection. Crit Care 24:500. https://pubmed.ncbi.nlm.nih.gov/32792018
- Zhang J, Rao X, Li Y et al. (2021) Pilot trial of high-dose vitamin C in critically ill COVID-19 patients. Ann Intenisve Care 11:5. https://pubmed.ncbi.nlm.nih.gov/33420963
- Lankadeva YR, Peiris RM, Okazaki N, et al. (2021) Reversal of the pathophysiological responses to Gram-negative sepsis by megadose Vitamin C. Crit Care Med 49:e179-e190. https://pubmed.ncbi.nlm.nih.gov/33239507
- Patterson G, Isales CM, Fulzele S. (2021) Low level of vitamin C and dysregulation of vitamin C transporter might be involved in the severity of COVID-19 infection. Aging and Disease 12:14-26. https://pubmed.ncbi.nlm.nih.gov/33532123
- Tomassa-Irriguible TM, Lielsa-Berrocal L. (2020) COVID-19: Up to 87% critically ill patients had low vitamin C values. Research Square, preprint. https://www.researchsquare.com/article/rs-89413/v1
- Arvinte C, Singh M, Marik PE. Serum levels of vitamin C and vitamin D in a cohort of critically ill COVID-19 patients of a North American Community Hospital Intensive Care Unit in May 2020. A pilot study. Medicine in Drug Discovery 8:100064. https://pubmed.ncbi.nlm.nih.gov/32964205
- Wagas Khan HM, Parikh N, Megala SM, Predeteanu GS. (2020) Unusual Recovery of a Critical COVID-19 Patient After Administration of Intravenous Vitamin C. Am J Case Rep 21: e925521. https://pubmed.ncbi.nlm.nih.gov/32709838
- Marik PE. (2018) Hydrocortisone, Ascorbic Acid and Thiamine (HAT therapy) for the treatment of sepsis. Focus on ascorbic acid. Nutrients 10:1762. https://pubmed.ncbi.nlm.nih.gov/30441816
- May JM, Qu ZC. (2011) Ascorbic acid prevents oxidant-induced increases in endothelial permeability. Biofactors 37:46-50. https://pubmed.ncbi.nlm.nih.gov/21328627
- Utoguchi N, Ikeda K, Saeki K et al. (1995) Ascorbic acid stimulates barrier function of cultured endothelial cell monolayer. J Cell Physiol 163:393-399. https://pubmed.ncbi.nlm.nih.gov/7706381
- Han M, Pendem S, Teh SL, et al. (2010) Ascorbate protects endothelial barrier function during septic insult: Role of protein phosphatase type 2A. Free Radic Biol Med 48:128-135. https://pubmed.ncbi.nlm.nih.gov/19840845
Orthomolecular Medicine News Service (OMNS) <omns@orthomolecular.org>
OMNS free subscription link http://orthomolecular.org/subscribe.html
OMNS archive link http://orthomolecular.org/resources/omns/index.shtml
Click here to see a web copy of this news release:
Published from: orthomolecular.activehosted.com
New Research Questions Use of Cryotherapy in Football Injury Recovery
New research has revealed a potential pitfall when it comes to the use of cryotherapy chambers to protect top flight footballers from injury. And the routine use of this extreme cold temperature treatment needs to be re-assessed. That’s according to new research led by experts from Liverpool Hope University, as well as the University of Central Lancashire and Edge Hill University.
Academics examined so-called ‘Whole-body cryotherapy’, or ‘WBC’, where players are exposed to icy temperatures between -110 C and -195 C for up to three minutes in a special liquid nitrogen-cooled chamber. It’s common throughout elite sport, and is said to aid recovery by stopping inflammation in its tracks, while also promoting the release of feel-good endorphins.
But Dr James Malone, Senior Lecturer in Coaching Science at Hope, has called for more research into the long-term effects of WBC. Over the course of almost two seasons, he followed a group of 16 Premier League players. Despite the players falling into three groups - ‘low’, ‘medium’ and ‘high’ cryo exposure - there was actually no difference in the player’s ‘recovery rates.
Dr Malone points out, the adage that ‘more is better’ may not be the case when it comes to WBC as higher doses had no additional benefit.
But what researchers did find is that one of the player groups displayed a ‘significant reduction’ in salivary immunoglobulin - aka ‘IgA’ - concentration post-match. That indicates a less than optimum immune system, and which could leave players open to infection while also having a knock-on effect on performance.
The results have been published this month in the journal Biology of Sport.
Dr Malone explains:
“Whole Body Cryotherapy is used to accelerate the recovery profile in players and this year it has been more important than ever before, with clubs enduring a more congested season and having had a limited pre-season.
“Clubs playing in Europe, such as Liverpool and Manchester City, often have matches twice a week, meaning recovery becomes much more important and fatigue becomes a real issue.
“And our findings suggest we actually need more research into the benefits of Whole Body Cryotherapy to aid this recovery.
“When the immune system is suppressed and IgA levels reduced, you see an increased risk of respiratory illnesses like colds and flu.
“If a footballer picks up an illness, they might be unable to train or play matches for a few days, having a huge knock-on effect for the team, while there’s also the risk of fatigue.”
Whole Body Cryotherapy first came to prominence in Rugby Union before spreading to other elite sports like football. It works in the same way as an ice bath might, reducing inflammation and alleviating pain in the body.
As Dr Malone adds:
“Cryotherapy works by reducing muscle damage induced soreness that we get post-exercise. This is usually in the form of inflammation within the muscle, with the extreme temperatures within cryotherapy acting as a ‘vasoconstrictor’ to limit this response.
“And Whole Body Cryotherapy is popular among players because they can enter the chamber for two to three minutes, rather than having to sit in an ice bath for 10 minutes, which can be pretty horrific if you’re not accustomed to it.”
The players being analysed were able to choose their own WBC regime, adjusting the temperature and duration to suit their preferences.
The ‘High’ group enjoyed an average temperature of -133 C and spent on average 181 seconds in the chamber, the ‘Medium’ group set the temperature at an average -121 C and spent roughly 173 seconds being frozen, and the ‘Low’ group opted for around -114 C and spend approximately 133 seconds undergoing WBC.
And, interestingly, it was the ‘Medium’ group whose immune system saw a reduction in virus-fighting immunoglobulins - a large 22 per cent reduction in the ‘Medium’ group compared with the ‘Low’ group.
(* IgA levels High - 306 micrograms per millilitre, Medium- 255 micrograms per millilitre, Low - 328 micrograms per millilitre).
In the journal, Dr Malone writes:
“A reduction in salivary IgA is seen as potentially detrimental to performance due to suppression of the immune system. This may lead to potential time-loss illnesses which can have a significant impact on squad availability, particularly during congested fixture periods such as the winter period in the English Premier League.”
So, why did the researchers see this effect in the ‘Medium’ group, in a ‘reverse Goldilocks’ scenario?
Dr Malone admits the team were intrigued, and notes:
“What we found was a U-shaped curve, where the middle group has a suppressed immune response yet both the low and high groups were actually fine.
“We were surprised by our findings, which suggest there’s an optimal level of whole body cryotherapy in terms of recovery and our results should prompt further research.
“You’d expect the middle level to be the most optimal - not too much or too little cryotherapy. But we actually found the opposite. And because it was such a long term study, backed with lots of data, we’re confident that it’s not some sort of statistical anomaly.
“At present we have no satisfactory explanation, namely as the majority of previous research has only looked at short term use of just a few days or a couple of weeks.”
While it wasn’t part of the present study, Dr Malone also questions whether Whole Body Cryotherapy is any better than the use of traditional ice baths.
Describing how the self-reported player wellness scores were almost identical between the three groups, he adds:
“The wellness scores, a subjective measure, can be sensitive to fatigue in footballers. But what’s interesting is that we actually didn’t find any difference in wellness scores between the three groups.
“Again, you’d expect the higher exposure group to have better scores. But what we found was that, regardless of dose, they pretty much all felt the same after a game. And this poses some important questions.
“When elite sport is constantly looking for that competitive edge, it can often be a case of ‘adopt first, research later’, and we need the data to back up the use of Whole Body Cryotherapy, as with all recovery methods we use.
“There’s also the question of cost. Whole Body Cryotherapy is not a cheap thing, costing around £80,000 plus to install, and maintenance is expensive, too.
“If you base your weekly recovery methods on the research, and not on player preference, it could be argued that cold water immersion - such as ice baths - is just as effective, overall, as it’s giving you the same sort of effect for a much reduced cost.
Further Information
You can read the full report here.
For further information or for interview requests please contact Hope journalist Neil Goodwin – goodwin@hope.ac.uk
About Liverpool Hope University
With a history extending more than 170 years, Liverpool Hope has a rich heritage that pre-dates many ‘red brick’ universities, but remains focused on the future.
The university has two main campuses- Hope Park, Childwall and the Creative Campus in Liverpool city centre. Both have seen major investment, so traditional architecture now sits beside contemporary buildings and facilities.
5 Things That Actually Cause Blood Clots
Over 11 million doses of the vaccine have been given across the UK, and the number of blood clots reported following vaccination isn't higher than the number of people that would've naturally got a blood clot in the vaccinated population. The European Union has approved the safety of the AstraZeneca vaccine after pausing the rollout, so it is safe to receive.
Any medication that goes into circulation is subject to rigorous testing – no corners are cut, no matter how urgent the need. In the 1950s, the thalidomide scandal resulted in tighter testing on drugs when tens of thousands of deformed babies were born when pregnant women were prescribed it, so it is understandable that concerns around vaccinations and drug prescriptions must be investigated.
Interest in blood clots has surged because of recent news. myGP looked at Google Trend data to find out what users were searching for – assigning a score from 0 to 100 based on interest, and 100 being the highest. According to the data, on 13th March 2021, interest scores for “blood clot symptoms” in the UK was 11, which is low. On the 15th March 2021, it had risen to 100. Similarly, the interest score for “AstraZeneca blood clot” in the UK was on 0 on 11th March and skyrocketed up to 100 on the 14th March.
Following reports of blood clots following the AstraZeneca vaccine for COVID-19, there was understandably a need for these to be investigated. However, it is important to acknowledge that the vaccine has since been approved again as "safe and effective" and concerns of blood clots were debunked.
If you’re concerned about the risk of blood clots, we’re here help give you accurate information about things that can contribute to blood clots, and how you can prevent them.
Smoking
Smoking can contribute to a vast majority of health problems, so it isn’t surprising that smoking cigarettes is on the list.
As well as damaging nearly every organ in your body, smoking is the leading preventable cause of disease and death. Smoking significantly increases your risk of blood clots and will contribute to platelets sticking together, which are small cell fragments in our blood that clot to prevent bleeding. Smoking damages blood vessel lining, which can cause clots to form.
Atherosclerosis can arise from smoking, where plaque in the blood builds and sticks to the artery walls. These plaques of blood make your arteries smaller which reduces blood flow and can lead to blood clots.
- aheart attack
- blockages
- stroke
- coronary heart disease
Tips to Stop Smoking
Quitting smoking can be difficult – after all, it is an addiction. However, don’t feel like you are a “lost cause” and that the damage has already been done. There is always time for you to better your health. Did you know that there are health benefits even after eight to 12 hours after quitting? Your blood carbon monoxide levels drop. Two to three weeks after quitting, your risk of heart attack drops. One year after quitting, your risk of heart disease will be cut in half. 10 years after quitting, your risk of lung cancer falls to the same level of someone who never smoked.
If you’re looking to stop smoking, be positive. Follow these NHS guidelines to put down the cigarettes for good:
- Make a realistic plan to quit smoking.
- Consider your diet. Some foods can trigger your cravings, for example, if you enjoy an after-dinner cigarette following a meat-heavy meal.
- Change what you drink. Juice and water make you less likely to crave a cigarette.
- Avoid situations where you enjoy smoking.
- Get support from friends, family, or healthcare workers. Call the NHS Smokefree helpline on 0300 123 1044.
- Exercise more.
- Keep your hands and mouth busy.
Contraception
Estrogen-based contraceptives can contribute to your risk of a blood clot. Not only the pill, but patches, injections, or vaginal rings that deliver estrogen to the blood stream can all cause an increased risk. Because of hormone changes, this can cause blood cells to form clots.
The risk of blood clots when on estrogen-based contraceptives is higher in:
- Those with a family history of blood clots.
- Those who have had surgery.
- Those who are obese.
- Those who go on prolonged travel.
Sometimes, the contraception we’re on best suits us. We might have fewer side effects on a specific type, we can access it easily and order prescriptions online, or generally prefer a certain method. To reduce your risk of blood clots while on estrogen-based contraception, you should:
- Maintain a healthy weight with diet and regular exercise.
- Drink enough water, particularly when travelling.
- Wear compression socks – get advice from your GP on this.
- Be aware of the symptoms – these may include chest pain, shortness of breath, upper body discomfort including int he arms, back, jaw, or neck, speech changes, paralysis, trouble speaking, and redness, pain, warmth, or swelling in the lower leg.
Pregnancy
Did you know that if you're pregnant or have recently given birth, you are at higher risk of blood clots? Pregnant women are five times more likely to have a blood clot than a woman who isn’t pregnant.
Due to changes a woman's body will go through, including less blood flow getting to the legs of pregnant women due to the pressure of a growing baby on the pelvis and limited mobility, this can increase the risk of blood clots.
You should speak to your doctor about your risk and if you have any and be aware of the symptoms.
Prolonged bed rest
Blood clots can arise due to prolonged bed rest. It is important to keep your blood flowing when you're immobile for a significant period of time. For example, if you're ill or are recovering from surgery, you need to keep your limbs active to encourage blood flow.
Compression stockings can also aid with this, designed to apply pressure to your legs to maintain blood flow.
COVID-19
Lastly, and most importantly – COVID-19. COVID-19 can cause blood clots, not the vaccination against it. Blood clots are seen in people who have been hospitalised with the virus. According to Healthline, 31 per cent of these patients had blood clot related complications – it isn’t just old people that are at risk, but young people too.
To reduce your risk, you can follow the tips discussed throughout this article, like maintaining a healthy weight, regularly exercising, drinking water, and avoiding smoking.
Sources
https://www.bbc.co.uk/news/world-europe-56440139
https://www.sciencemuseum.org.uk/objects-and-stories/medicine/thalidomide
https://patient.info/news-and-features/astrazeneca-vaccine-is-it-safe-and-does-it-cause-blood-clots
https://ash.org.uk/wp-content/uploads/2019/10/FactsataGlance.pdf
https://www.healthline.com/health/effects-of-quitting-smoking#quitting-timeline
https://www.nhs.uk/live-well/quit-smoking/10-self-help-tips-to-stop-smoking/
https://www.cdc.gov/ncbddd/dvt/features/blood-clots-pregnant-women.html
Source and Acknowledgement Citation
Comments:
-
No Article Comments available