Positive Health Online
Your Country

![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Organic Aromatherapy]](/img/original/TopicbannerAvatar/1001.12a011c5d14492e86a5a2fa985244b74.jpg "Organic Aromatherapy")
![[Image: Human Kinetics Trail Guide to the Body]](/img/original/TopicbannerAvatar/4656.d9ccc329faa3d1500b4807b369feccef.jpg "Human Kinetics Trail Guide to the Body")
![[Image: ICAN International Clinical Aromatherapy Network]](/img/original/TopicbannerAvatar/4442.566a83a07de79de73b9c738f7fb6458a.jpg "ICAN International Clinical Aromatherapy Network")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
![[Image: SG Cancer Book]](/img/original/TopicbannerAvatar/960.4f24bbd158abe4427cc06911969143e5.jpg "SG Cancer Book")
Blueprint to Healthy Eating, Fuelling and Exercising
by Dr Robert Verkerk(more info)
listed in nutrition, originally published in issue 223 - July 2015
Eating a healthy and balanced diet is key to improving the quality of your life, especially when coupled with regular physical activity and due attention to your emotional health, right? But when it comes to food composition, what should we be eating? In this piece, we outline why government guidelines simply don’t stack with current nutritional science and we offer our alternative, Food4Health guideline plate. We also discuss the importance of metabolic flexibility and resilience, and take a look at how we use and store the energy in the body.
Any guideline, whether from governments or other organizations, are a crude yardstick. They should be seen as something of a starting point or a rough guide, not a ‘bible’. They should allow choice and flexibility, especially to take into account huge differences between individuals in relation to their needs and genetics. Fine-tuning over time is generally needed, a process that can sometimes take years before you find your body’s really singing! But, by contrast, if your food composition and frequency is out of kilter, getting it back into balance can deliver benefits that can be felt in a matter of days.
Government Health Warning
In 2010, the UK’s Food Standards Agency (FSA) revised its Eatwell Plate guidelines. The guidelines are intended to help the average person “eat a healthier diet” which is intended to reduce their long-term risk of chronic diseases like obesity, type 2 diabetes, heart disease and cancer. With governments facing the same network of Big Food and Big Ag interests, the advice ends up much the same the world over. That’s why the US MyPlate guidance has many of the same recommendations as the UK Eatwell guidelines.
The continuing spiral of chronic diseases tells us either that people are not heeding government guidelines or they are not appropriate. A growing evidence base, especially the effects of consuming excess starchy carbs and insufficient healthy fats and protein, would suggest that the latter is a significant factor at least.
Top Down - Only Part of the Solution
Attempts at getting the public to eat the right things and reduce obesity and the burden of chronic disease have a spectacular history of failure. The EU’s five-year obesity strategy (2007-12) is one such failure. In the UK, the Public Health Responsibility Deal that aims to make manufacturers more responsible is now being rolled out with great gusto. Among the Responsibility Deal’s broadcasted successes are Big Food’s reduced sugar breakfast cereals, reducing the amount of alcohol on the market by a billion units, tips for healthier eating at take-aways, and Britvic’s decision to remove its full sugar Fruit Shoot from the market.
History tells us these kinds of top-down changes don’t dramatically change people’s approach to nutrition and activity sufficiently to create a turn-around in health. Hence the guideline food plates – but they are again little more than a compromise that have been decided between industry and government.
‘Ten Terrible Tips’ in Government Guidelines
During deliberations with integrative medicine practitioners and nutrition science researchers over the last decade and a half, along with our continual review of the literature, we have consistently had our attention brought to problems with the government guidelines. We’ve selected the 10 ‘terrible tips’ that are consistently raised:
- Starchy carbs are massively over-recommended
- The effect of food processing technologies and cooking on glycaemic load is generally ignored
- Low-fat is still advocated, despite it often being linked to diets high in refined carbs and sugars
- Grains (e.g., cereals, bread, pasta) are recommended as the primary source of energy, despite numerous problems, especially with wheat and gluten, ranging from coeliac disease, leaky gut syndrome, non-coeliac gluten-sensitivity and numerous other related gastro-intestinal and autoimmune conditions
- Helping individuals out of food addiction, especially the combined effect of sugar and particular fats, is not adequately taken into account. This issue was graphically illustrated by a BBC experiment on doctor twins, Alexander and Chris and van Tulleken
- There is inadequate emphasis placed on certain food groups, such as healthy fats and concentrated nutrients such as in herbs and spices
- There is little or no consideration of meal/food frequency
- There is little or no consideration of processing, preparation or cooking methods
- There is no provision for supplements, despite evidence of their value in many sub-populations (e.g. Omega-3 fatty acids, vitamin D, multivitamin/minerals, etc.)
- Governments push dairy products to ensure sufficient calcium is consumed. Evidence shows that calcium is not normally deficient in the diet, but co-factors are, such as vitamin D, vitamin K2, magnesium and other nutrients. Humans did not evolve to consume large quantities of milk from other animals and lactase deficiency is exceedingly common in some adult populations, ranging from 45-100% in Latin-American populations, to around 90% in Japanese.
The Road to New Guidelines
Coupling the most relevant published science with clinical experience gives us the basis for making dietary recommendations and is where the integrative medicine sector, for want of a better name, is in a unique position to provide guidance. As far as we are aware, it is the only sector that is consistently having clinical success treating and preventing chronic disease using dietary interventions. It also routinely has success helping obese individuals to lose weight – and keep it off, even when they are so-called ‘non-responders’. The sector is strongly plugged into, and plays a key role in, pushing forward the boundaries of nutritional science.
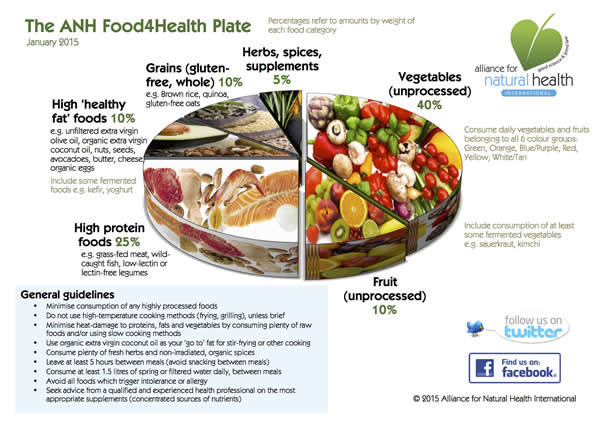
The ANH-Intl Food4Health Plate
Earlier this year, we released the ‘ANH Food4Health Plate’. It gives an approximate distribution of the percentage by weight of daily consumption of key food groups. However, our guidelines use a different system of categorization of food groups compared with government guidelines. Critical to our health is the relative amounts and quality of macronutrients, as well as micronutrients, along with the state of these at the point they enter our bodies.
In essence, our plate looks like this by weight:
- 40% unprocessed veg
- 10% unprocessed fruit
- 25% high protein foods
- 10% healthy fat foods
- 10% whole grains (gluten-free)
- 5% concentrated nutrients in the form of fresh herbs, supplements, etc.
We’ve factored in various food combinations that fit this pattern and a typical macronutrient composition - still by weight - looks something like this:
- 32% protein, mainly from meats (where present), veg, nuts/seeds, cheese/dairy (where present), etc.
- 28% fats, mainly from oils, seeds, nuts, oily fruits like avocado, and from meats (where present)
- 40% carbohydrates, mainly from veg, fruits and grains (where present)
Looking again at the above macronutrient ratios from an energy contribution viewpoint gives the following approximate ratios:
- 24% protein
- 46% fat
- 30% carbohydrate.
This contrasts with UK guidelines that suggest 50% of energy should come from carbohydrates, whereas we are suggesting around 50% should come from fat. A paper just out in the journal Open Heart has proven that the low fat guidelines developed by the UK and US governments in the 1970s and 1980s had no scientific basis and were wrong, even with the knowledge available then. With today’s knowledge, it’s verging on criminal.
Example Plate
Following is a main meal including a salad that roughly fits the Food4Health Plate guideline. It includes some lean protein, healthy fats, lots of veg, a small portion of brown rice, some fruit and some nuts. What you’ll see is that more than half (57%) of the energy in it comes from fats and less than 20% comes from carbs. A day's eating, rather than just this one meal, would likely include a bit more fruit and veg that would likely bring the carb contribution closer to the 30% mark mentioned above.
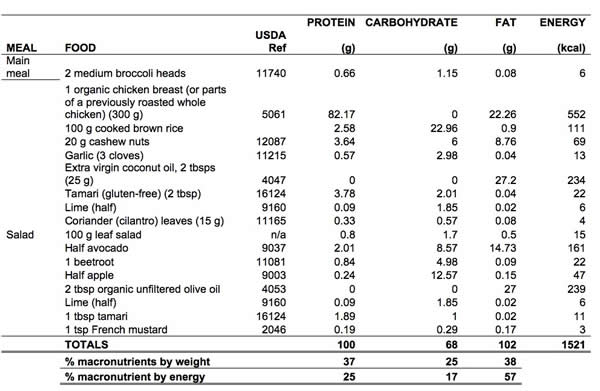
Table 1. Example plate, roughly consistent with the ANH Food4Health Plate guidelines
(data source: USDA National Nutrient Database)
So when you look at our one-meal plate in terms of weights, it might look like a low fat plate. But it isn’t, as you’ll see from the calculation according to energy contribution. There’s a fair bit of healthy fats coming in from all the food groups and because of the energy contribution of fats, more than doubling that of proteins and carbs, you end up with a relatively high fat content. If you are extremely active, being for example an endurance athlete, you might end up benefiting from closer to 80% of your energy from fats! But you need to be keto-adapted, highly active and have no insurmountable genetic impairments in your ability to metabolize fats to do that.
So our plate, like any plate, is still a compromise, built around the average person that remains little more than a statistical artefact.
So Much More than What’s on your Plate
Alongside what you eat, we have to consider how and when you eat, and it is now widely recognized that the snacking culture not only contributes to excess calories, but also promotes low-grade inflammation that is at the basis of most chronic diseases. How you prepare your food, how you chew it, when you eat, how long you leave between meals, along with your genetic background, lifestyle, physical activity and nutritional needs, are all crucial to deciding how the food will interact with your metabolism. Fasting for 12 hours overnight and 5 hours between meals, as proposed by the Metabolic Balance programme, is achievable for most people, albeit requiring a bit of self-discipline in the early stages of becoming a ‘non-snacker’. Intermittent fasting has helped many tens of thousands to reset their metabolism and endocrine system, helping people to emerge from insulin resistance, pre-diabetes, metabolic syndrome and even clinical type 2 diabetes. Eating little and often, as recommended by the vast bulk of dieticians, simply pushes people into insulin resistance and a downward spiral of associated metabolic diseases that now plague our society.
Guideline Food Plates: yes or no…
Anyone who says “they’re all useless” would pique my interest. As we’ve said above, no one plate will suit everyone. Even any one individual - say you or me - shouldn’t eat the same composition of foods and macronutrients (protein, fats and carbs) every day, day in day out. That’s because our activity pattern, stress and other elements of our lifestyle are, or should be, in a continuous state of flux.
This brings us to two key points: metabolic flexibility and resilience. These are the real markers of health. Metabolic flexibility refers to the capacity to adapt to, and burn (oxidize), whichever fuel is available. Someone who has developed metabolic flexibility can therefore handle a more variable diet and can burn fats effectively, these being the richest source of energy for the body. Physiological resilience refers to your ability to respond and recover from physiological, metabolic, immunological or lifestyle stress. Someone who is resilient, is someone who can regain equilibrium - or homeostasis - more quickly than someone who may be free from clinical symptoms of disease, but ultimately, lacks this supreme level of vibrant, resilient, and ultimately, adaptive health.
What principles mean that someone has obtained a state of metabolic flexibility and resilience?
- They are keto-adapted and are able to readily burn fats for fuel;
- They regularly practise caloric restriction (intermittent fasting) through fasting between meals. This is quite different from just eating fewer calories every day, little and often!
- They are physically active (at least 1-2 hours moderate activity/day);
- Their diet is anti-inflammatory and loaded with phytonutrients from the 6 main colour groups of the phytonutrient spectrum;
- The bulk of their diet, in terms of its energy contribution, does not come from carbohydrates - wholegrain or otherwise!
- They show no signs of metabolic syndrome or insulin resistance, either in muscles or in other tissues and therefore have ideal or near-ideal body compositions (muscle/adipose/visceral fat ratios);
- They have modified their nutritional intake, eating habits and lifestyle in such a way as to largely offset any disadvantageous genetic limitations or polymorphisms they may carry;
- Their diet and activity levels create psychoemotional flexibility too, meaning more emotional balance – and yes, happiness!
Fuel Efficiency and the Food4Health Plate
If you're keen on living naturally, and minimizing your risk of chronic disease in later life, it’s very important to understand something about the ways in which we burn food as fuel - and how we store our fuels. Doing this right will help you to become - or stay - lean and fit, while reducing burden on the healthcare system and especially unnecessary use of pharmaceutical medicines. Call it ‘personal responsibility in health’, ‘disease prevention medicine’, or plain old ‘staying fit and healthy’. It’s about helping you to take back control of your health, in the event you might have already handed that responsibility to someone else, or are concerned that, later in life, that responsibility may be wrestled from you.
How Do You Burn Your Fuel?
Over millennia, our bodies have developed very intelligent systems for:
- Turning the food we eat into the energy we need to run all of our internal metabolism;
- Building new DNA and cells;
- Running our brains and immune systems (that are among the two biggest energy sinks we have);
- Digesting our food;
- Fueling our mitochondria and muscles.
Carbs
Anaerobic glycolosis: Carbs are basically long chains, simple or complex, of glucose. We get energy out of glucose (a 6-carbon sugar) by splitting each molecule into two 3-carbon sugars. We refer to this process as glycolysis, which literally means ‘sugar splitting’. In the absence of oxygen (anaerobic glycolysis) every molecule of glucose generates, via a series of enzyme-controlled steps, a limited amount of energy in the form of two molecules of ATP (adenosine triphosphate). But it also produces two molecules of pyruvic acid (pyruvate). Still in the absence of oxygen, such as when you’re exercising for extended periods close to your maximum limit, you start to ferment this pyruvate, yielding lactic acid (Fig. 1).
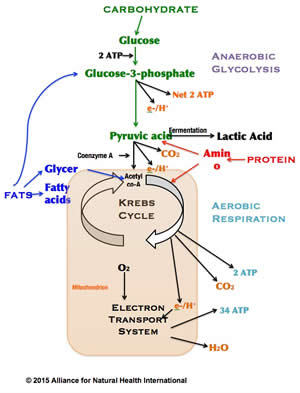
Figure 1. Key anaerobic and aerobic pathways for cellular respiration of macronutrients
While ATP is the primary fuel used for most reactions in the body most of the time, this small amount of energy from anaerobic glycolysis is used mainly to produce energy carriers like NADH and FADH2.
Let’s not forget, we need a lot of ATP, about half or more of your body weight’s worth daily! Some of this we get from our food, some we get by recycling ATP. We get energy from ATP by breaking the high-energy bond in the molecule when one of its phosphorus groups is enzymatically cleaved from it so forming ADP (adenosine diphosphate). We can then use energy from our food, produced in the mitochondria, to convert the ADP back to ATP.
Aerobic glycolysis: Put oxygen into the equation and it’s a very different story. Aerobic glycolysis occurs when you are not exercising near your limit and exceeding your lactate threshold. Here, the pyruvate is used, following its conversion to acetyl co-enzyme A (acetyl-coA), a key substrate for the Kreb’s (citric acid) cycle in the energy-generating factories we have in cells, especially muscle cells, called mitochondria. You may only get 2 ATP molecules directly from Krebs (also used mainly to generate energy carriers), but Kreb’s metabolites, along with various cofactors including coenzyme Q10, then set off the proton gradient that yields the bulk of mitochondrial energy in the electron transport system (ETS). This is the main way we get energy from carbs, proteins and fats. And when we oxidize glucose, we get a somewhat impressive 34 molecules of ATP for each molecule of glucose.
Another point is that we can store glucose, but not very much of it. We do this in the form of glycogen. We can store around 100 grams of glycogen in the liver and about 400 grams in the muscles. Most people have burned this up after around 90 mins of strenuous activity in the absence of other fuel. That’s also why longer bouts of moderate activity can be so effective at burning fat.
Proteins
Proteins also get oxidized to form energy in the form of ATP. What is key to appreciate is that the oxidation of proteins and fats, as seen in Figure 1, also converge on the Kreb’s cycle. In the case of proteins, they must be oxidized to their constituent amino acids (of which there are 20 in total), and have their nitrogen removed in order to become substrates that are used directly or indirectly in the Krebs cycle. These reactions that allow inter-conversion between amino acids and energy substrates are called transamination and deamination reactions. Glutamate is also a critical player because it is the key transporter of amino acids in the blood, while exerting other key functions such as helping to maintain integrity of the intestinal lining and supporting the immune system and kidneys.
Gram for gram, protein yields about the same amount of energy as carbohydrates. That’s one of the reasons food labelling laws require that manufacturers stipulate that 4 calories (kcal) are yielded for every gram of carb or protein contained in a food. Actually that’s the case if you both absorb and oxidize the fuel fully. The latter is usually determined on a lab bench using a bomb calorimeter. The problem is many people don’t digest, absorb or oxidize their fuels fully because of one or more impairments, these being genetic or physiological.
Fats
Let’s leave the best to last! Fats yield energy from oxidation too and the products of oxidation, just like carbs and protein, converge on the Kreb’s cycle. Fats are broken down to their constituent fatty acids via the beta-oxidation pathway, mainly in the liver. They then yield the common denominator acetyl-coA via 4 reactions that occur again in the mitochondria (and peroxisomes), mainly in the liver and muscles.
If you take just one molecule of a fatty acid, say palmitate, you can generate a stunning theoretical yield of 129 ATP molecules using the beta-oxidation pathway! This makes even the 34 ATP yield from aerobic glycolysis from a glucose molecule look somewhat paltry.
Nutritional Ketosis
But that’s not all. If the amount of carbohydrate consumed is limited, especially while the energy requirement is increased (i.e. as a result of exercise), more acetyl-coA will be produced from the beta-oxidation of fatty acids. If there is more than is required to meet the energy needs of an individual, this excess acetyl-coA will be shunted into another process called ketogenesis, that yields ketone bodies (acetoacetate, β-hydroxybutyrate and acetone). These then become an additional metabolic fuel.
From an evolutionary perspective, this pathway has been vital to human success and is clear evidence for just how well we are adapted to starvation and what we now think of as ‘intermittent fasting’ (i.e. NOT three meals a day with snacks in between). Without carbs, proteins and fats from our food, in other words during starvation, we can actually use ketone bodies produced by beta-oxidation of our own fat deposits as our primary fuel for vital organs such as the brain and heart. Do it for too long and raise your ketone levels too high, you….die. A good enough reason to ensure starvation is not maintained!
For a long time, scientists and doctors thought of ketosis, the process that generates ketone bodies, as a bad thing. That’s because it was associated with either starvation, or uncontrolled diabetics, who can develop serious and life-threatening diabetic ketoacidosis. When ketone bodies develop excessively in the body you can smell a strong, characteristic fruity, pear drop smell on the breath. This is the result of high levels of acetone being produced.
As shown by Drs Jeff Volek and Steve Phinney in their bestselling book, The Art and Science of Low Carb Living, healthy, nutritional ketosis is established when serum (blood) concentrations of ketone bodies are in the range 0.5-3.0 mM. This is what they refer to as the “optimal ketone zone” and can be achieved with a low carb, relatively high fat, ketogenic diet, such as that consumed when you follow the Food4Health Plate.
As far as storage and use of proteins and fats are concerned, if we don’t have enough carbs in our body, and we haven’t adapted to burning fats because we have not yet adapted to switching to the fatty acid-burning beta-oxidation pathway, we can start burning protein, especially in muscles. This is never a good thing, especially if you’re interested in improving your lean muscle mass and being physically very active.
We’re all aware of how readily we store energy as fat. We also know that the main reason people get fat is not from eating too much fat, but by eating too little - and too much carbohydrate. Fat can exist in many forms and is stored in different ways and places including beneath the skin (as adipose tissue) or around the organs (as visceral fat). Generally the latter is the most dangerous and needn’t be that visible, hence recent concerns about the risk of being ‘skinny fat’ i.e. thin on the outside, fat on the inside. This, once again, an increasingly common predicament triggered by low fat recommendations which have led to dependence and addiction to refined carbs from soft drinks, white bread and other ultra-processed, high glycaemic foods.
A bit of brown adipose tissue (BAT) or brown fat, on the other hand, is the healthiest fat to lay down. It becomes a key fuel if you are both keto-adapted and want the stamina of an endurance athlete.
Getting Flexible Nutritionally and Physically
Nutrition is of course just one of the pillars of health and wellness. You shouldn’t forget to exercise regularly and manage your emotional health. Getting the relationship between eating and physical activity right is a minefield, especially taking into account patterns of activity and genetic variations between individuals. But we have all learned a great deal about these complex interactions from successful sports physiologists and nutritionists, and a few central themes are beginning to emerge that apply to most people.
We’ve looked so far at how the body uses different types of fuel. What we now have to understand is that physical activity and exercise has a huge bearing on how this happens. In essence, the body is able to use one of three different energy systems while you exercise. Let’s look at these briefly in turn.
The Phosphagen, Creatine Phosphate or Phosphocreatine System
If you exercise extremely vigorously for a few seconds, such as when you break into a sprint or you trigger your fight or flight response, you don’t use ATP from cellular respiration. Instead, you rely on producing ATP, the universal fuel, from creatine phosphate of which you have very limited reserves in muscles. Its plusses are that it makes energy instantly. Its downside is it doesn’t make very much. So while it very effectively gets cyclist Mark Cavendish across the finish line in first place, the phosphagen system was there to originally protect us from sabre-toothed tigers.
The Anaerobic Glycolysis Pathway
This energy system we discussed earlier (Fig 1). It’s about making energy from glucose in the absence of oxygen. It can’t be sustained for more than about 5 minutes or so before the lactate accumulates excessively. Cramp is one outcome of being anaerobic too long.
The Aerobic Pathway
This is the key one for long-term energy use. It lets us burn any of the three major macronutrient fuels. But it’s the fats that are both the cleanest burning and, as we’ve seen above, yield by far the most energy. That’s why people are waking up to easy-access fatty fuels like virgin coconut oil, a very rich source of medium-chain triglycerides.
Transitioning from being a Carb Burner to a Fat Burner
The ease by which you can shift from being primarily reliant on carb burning, as compared with being a keto-adapted, fat burner, varies considerably in different people. There are a number of key practical steps you can take that will often have a dramatic effect in your transition:
- Avoid snacks of any type between meals, especially ones that are rich in simple carbs. (It’s okay to drink water);
- Maintain at least a 12-hour overnight fast on at least 5 days a week;
- Leave it at least 5 hours between meals or any form of food intake to allow the body to fast and avoid pushing it into low-grade inflammation;
- If possible, engage in high intensity physical activity for short periods (say 15 to 45 minutes) around twice weekly. This is often best carried out in the form of high intensity interval training (HIIT);
- Engage in some periods - say three times a week - of longer, lower intensity endurance exercise (in excess of 1.5 hours on each occasion) to help the body move into beta-oxidation of fats after muscle and liver glycogen has been depleted. For most people, this can be done at around 55-75% of your maximal heart rate. Avoid popping energy gels or other sources of carbohydrate during these sessions as they will switch off fat burning;
- Consume at least 25 g of protein and perhaps 5 g of glutamine and 5 g of branched-chain amino acids within a 30 minute window following completion of intense exercise to help your muscles to recover;
- Stretch those muscles that have been worked carefully after bouts of intense and extended exercise;
- Rest sufficiently between bouts of exercise, so that your muscles can rebuild and compensate following the damage caused by the exercise which in turn acts as a trigger to build bigger, stronger and leaner muscle.
Planning for Health
Getting the balance between your nutritional intake and your physical activity regime right is both an art and a science. Keeping a food and training diary can be very helpful, as can monitoring your progress in various physical pursuits.
Integrating these approaches into your life is the best way of experiencing a very high level of vital health. However, that’s easier said than done given time and other constraints that apply to so many of us.
The point is doing something right is always better than doing nothing right. So make a start….today!
Bibliography
1. Colagiuri S et al. The Metabolic Syndrome: from inherited survival trait to a health care problem. Exp Clin Endocrinol Diab 105 suppl 2: 54-60. 1997.
2. Cordain L et al. Origins and evolution of the Western diet: health implications for the 21st century. Am J Clin Nutr Feb 81(2): 341-54. Review. 2005.
3. Cordain L et al. Modulation of immune function by dietary lectins in rheumatoid arthritis. Br J Nutr 83(3): 207-17. Review. 2000.
4. Cordain L et al. The paradoxical nature of hunter-gatherer diets: meat-based, yet non-atherogenic. Eur J Clin Nutr 56 Suppl 1: S42-52. Review. 2002.
5. Cordain L. Cereal grains: humanity's double-edged sword. World Rev Nutr Diet 84: 19-73. Review. 1999.
6. De Lorgeril M et al. Effect of a Mediterranean Type of diet on the rate of cardiovascular complications in patients with coronary artery disease. JACC 28(5): 1103-1108. 1990.
7. Eaton SB Cordain L. Evolutionary aspects of diet: old genes, new fuels. Nutritional changes since agriculture. World Rev Nutr Diet 81: 26-37. Review. 1997
8. Eaton SB et al. Evolution, body composition, insulin receptor competition, and insulin resistance. Prev Med 49(4): 283-5. 2009. Erratum in: Prev Med 52(1): 95. 2011 Jan.
9. Feinman RD et al. Dietary carbohydrate restriction as the first approach in diabetes management: critical review and evidence base. Nutrition 31(1): 1-13. 2015.
10. Fleming J et al. Endurance capacity and high-intensity exercise performance responses to a high fat diet. Int J Sport Nutr Exerc Metab 13(4): 466-78. 2003.
11. Jones JL et al. A Mediterranean-style low-glycemic-load diet improves variables of metabolic syndrome in women, and addition of a phytochemical-rich medical food enhances benefits on lipoprotein metabolism. J Clin Lipidol 5(3): 188-96. 2011
12. Leite JO et al. Low-carbohydrate diet disrupts the association between insulin resistance and weight gain. Metabolism 58(8): 1116-22. 2009.
13. Leite JO et al. Low-carbohydrate diets reduce lipid accumulation and arterial inflammation in guinea pigs fed a high-cholesterol diet. Atherosclerosis 209(2): 442-8. 2010.
14. Ludwig D et al. High glycemic index foods, overeating and obesity. Pediatrics 103(3): E26-E31. 1999.
15. O'Keefe JH Jr et al. Cardiovascular disease resulting from a diet and lifestyle at odds with our paleolithic genome: how to become a 21st-century hunter-gatherer. Mayo Clin Proc 79(1): 101-8. Review. 2004.
16. Ornish D. Can lifestyle changes reverse coronary heart disease? Lancet 336: 129-133. 1990.
17. Pan DA et al. Dietary fats, membrane phospholipids and obesity. J Nutr 124: 1555-1565. 1994
18. Paoli A et al. Beyond weight loss: a review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. Eur J Clin Nutr 67(8): 789-96. 2013.
19. Prasad AN et al. Diet therapy of epilepsy in the nineties; renewed experience with the ketogenic diet. Nutr Res 18(2): 403-416. 1998.
20. Pruimboom L et al. Lactase persistence and augmented salivary alpha-amylase gene copy numbers might have been selected by the combined toxic effects of gluten and (food born) pathogens. Med Hypotheses 82(3): 326-34. 2014.
21. de Punder K, Pruimboom L. The dietary intake of wheat and other cereal grains and their role in inflammation. Nutrients 5(3): 771-87. 2013.
22. Ramsden CE et al. Dietary fat quality and coronary heart disease prevention: a unified theory based on evolutionary, historical, global, and modern perspectives. Curr Treat Options Cardiovasc Med 11(4): 289-301. 2009.
23. Rasmussen OW et al. Effects on blood pressure, glucose and lipid levels of a high-monounsaturated fat diet compared with a high-carbohydrate diet in NIDDM subjects. Diab Care 16: 1565-1571. 1993.
24. Ruiz-Núñez B et al. Lifestyle and nutritional imbalances associated with Western diseases: causes and consequences of chronic systemic low-grade inflammation in an evolutionary context. J Nutr Biochem 24(7): 1183-201. 2013.
25. Sharman MJ et al. A ketogenic diet favorably affects serum biomarkers for cardiovascular disease in normal-weight men. J Nutr 132(7): 1879-85. 2002.
26. Sharman MJ Volek JS. Weight loss leads to reductions in inflammatory biomarkers after a very-low-carbohydrate diet and a low-fat diet in overweight men. Clin Sci (Lond) 107(4): 365-9. 2004.
27. Spiller G et al. Nuts and plasma lipids: An almond-based diet lowers LDL-C while preserving HDL-C. J Am Coll Nutr 17(3): 285-290. 1998.
28. Valencia M et al. The Pima Indians in Sonora, Mexico. Nutr Rev 57: S55-S58. 1999.
29. Volek J et al. Comparison of energy-restricted very low-carbohydrate and low-fat diets on weight loss and body composition in overweight men and women. Nutr Metab (Lond) 1(1): 13. 2004.
30. Volek JS et al. Diet and exercise for weight loss: a review of current issues. Sports Med 35(1): 1-9. Review. 2005.
31. Volek JS et al. Fasting lipoprotein and postprandial triacylglycerol responses to a low-carbohydrate diet supplemented with n-3 fatty acids. J Am Coll Nutr 19(3): 383-91. 2000.
32. Volek JS, Feinman RD. Carbohydrate restriction improves the features of Metabolic Syndrome. Metabolic Syndrome may be defined by the response to carbohydrate restriction. Nutr Metab (Lond) 2: 31. 2005.
33. Volek JS, Noakes T, Phinney SD. Rethinking fat as a fuel for endurance exercise. Eur J Sport Sci 15(1): 13-20. 2015.
34. Volek JS, Sharman MJ. Cardiovascular and hormonal aspects of very-low-carbohydrate ketogenic diets. Obes Res 12 Suppl 2: 115S-23S. Review. 2004.
35. Volek JS, Sharman MJ. Cardiovascular and hormonal aspects of very-low-carbohydrate ketogenic diets. Obes Res 12 Suppl 2: 115S-23S. Review. 2004.
36. Westman EC et al. Insulin resistance from a low carbohydrate, high fat diet perspective. Metab Syndr Relat Disord 3(1): 14-8. 2005.
37. Westman EC et al. A review of low-carbohydrate ketogenic diets. Curr Atheroscler Rep 5(6): 476-83. Review. 2003.
38. Wood RJ et al. Effects of a carbohydrate-restricted diet with and without supplemental soluble fiber on plasma low-density lipoprotein cholesterol and other clinical markers of cardiovascular risk. Metabolism 56(1): 58-67. 2007.
39. Yam D et al. Diet and disease - The Israeli Paradox: Possible dangers of a high Omega-6 poly unsaturated fatty acid diet. Isr. J Med Sci 32: 1134-1143. 1996.
Comments:
-
joanne frame said..
Thankyou very much for this article. Occasionally in my life I read something that intuitively I know is true, but it flies in the face of what I 'have been taught' This informative piece about nutrition is one of these times. A large anoutnt of carbohydrate always makes me feel heavy and bloated and put on weight. The times when I have followed a similar protocol to the diet described here I have felt healthy and have had a balanced weight. Its great to hear that there is scientific backing! I look forward to this awareness becoming more mainstream- in recipes and restaurants. I think if people started to follow tihs type of diet we would all feel a lot more alive :-)