Positive Health Online
Your Country

![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Lotus Books]](/img/original/TopicbannerAvatar/953.adb373b0210368e0c9ce4d9a8a9f01aa.jpg "Lotus Books")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
Muscle Energy Technique (MET)
listed in osteopathy, originally published in issue 214 - May 2014
Introduction
To understand the rationale behind MET it is first necessary to look at the mechanism that controls muscle tone. Sensory signals enter the cord via the sensory roots. After entering the cord sensory signals travel to two separate destinations.
- First either in the same segment of the cord or in nearby segments, the sensory nerve or its collaterals terminate in the grey matter of the cord and elicit local segmental responses (local excitatory / facilitatory effects and reflexes);
- Second the signals travel to higher levels of the nervous system to higher levels in the cord itself, to the brain stem and cerebral cortex.
Motor signals from the anterior motor neurons, leave the cord via the anterior roots and innervate the skeletal muscle fibres of which there are two types;
- Alpha a motor neurons of which stimulation of a single nerve fibre excites from 3 to 2000 skeletal muscle fibres which we call the motor unit.
- Gamma c motor neurons, which transmit impulses to special skeletal muscle fibres, called intrafusal fibres, part of the muscle spindle.
Most of the sensory fibrils entering each segment of the spinal cord terminate on interneurons
But a small number of large sensory fibres from the muscle spindles terminate directly on the anterior motor neurons. Thus there are 2 pathways in the spinal cord reflexes can take.
- Monosynaptic pathways provide an extremely rapid reflex feedback system and are the basis for the muscle stretch reflex;
- Polysynaptic pathways modify the signals greatly and can cause complex reflex patterns e.g. the protective or withdrawal reflex.
Muscles and Tendons have an abundance of two special types of receptors.
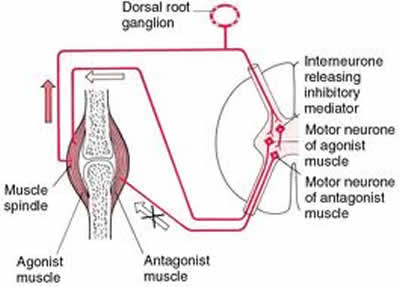
1. Muscle spindles that detect change in muscle fibre length & rate of change in length. Each muscle spindle is built around 3-10 small intrafusal muscle fibres attached to the sheaths of the surrounding extrafusal skeletal muscle fibres, the ends of which are excited by small gamma efferent motor nerve fibres.
The receptor portion of the muscle spindle is located midway between its to ends where the intrafusal muscle fibres have no contractile element. Sensory fibres originate in this area and are stimulated by stretch of this mid-portion of the spindle. These are the primary & secondary endings.
When the receptor portion of the muscle spindle is stretched slowly, the number of impulses transmitted from both the primary & secondary endings increases virtually in proportion to the degree of stretch. This effect is known as static response. The primary endings have a strong dynamic response, which means it responds very actively to a rapid change in length.
Muscle spindles emit sensory nerve impulses all the time when they are stretched the rate of firing increases, when they are shortened the rate of firing decreases. Its function is manifested in the form of the muscle stretch reflex, which consists of static & dynamic reflexes. The dynamic stretch reflex is caused by the potent dynamic signal transmitted via the primary endings of the muscle spindles. Therefore when a muscle is suddenly stretched a strong signal is transmitted to the spinal cord causing an instant v strong reflex contraction of the same muscle from which the signal originated. With the dynamic stretch reflex over within a few a fraction of a second after the muscle has been stretched to its new length, a much weaker static reflex continues after for as long as the muscle is maintained at an excessive length.
If the muscle is already taut any sudden release of the load on the muscle that allows it to shorten will elicit both dynamic & static reflex muscle inhibition rather than reflex excitation. Thus this negative stretch reflex opposes the shortening of the muscle in the same way that the positive stretch reflex opposes lengthening of the muscle. Whenever signals are transmitted from the motor cortex to the alpha motor neurons, the gamma motor neurons are stimulated simultaneously. This causes both the extrafusal & intrafusal muscle fibres to contract at the same time. Similarly these reflexes can be obtained from almost any muscle of the body by striking its tendon, i.e. eliciting a knee jerk. Thus sudden stretch of muscle spindles is all that is required to elicit a stretch reflex.
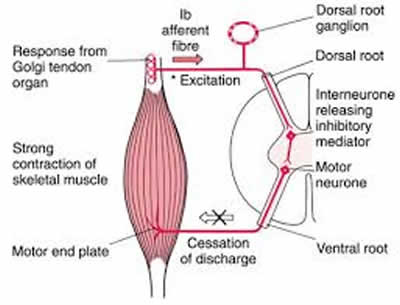
1. Golgi Tendon Organs that detect tension applied to the muscle tendon during muscle contraction/stretch. They lie within the muscle tendons. An average of 10 –15 muscle fibres are usually connected with each Golgi Tendon Organ (GTO) which are stimulated by tension from the muscle fibres. Thus the major difference between the GTO and the muscle spindle is the spindle detects relative muscle length & the GTO detects muscle tension. The GTO also has dynamic and static responses.
The GTO provides the nervous system with feedback on the degree of tension within each small segment of muscle. When they are stimulated by increases in muscle tension, signals are transmitted into the spinal cord causing an inhibitory reflex (exact opposite to a muscle spindle) resulting in muscle relaxation. This reflex thus provides a negative feedback mechanism that prevents the development of too much tension in the muscle. Therefore when tension on the tendon becomes extreme the inhibitory effect of the GTO can cause sudden relaxation of the entire muscle.
When a stretch reflex excites one muscle it simultaneously inhibits the agonist muscles, which is called reciprocal inhibition this takes place due to reciprocal innervation. Without this it would be impossible to move from say internal to external rotation.
Some muscle cramps result from a local irritating factor/metabolic abnormality such as severe cold, reduced blood flow, or excess exercise of the muscle. These can elicit pain or other types of sensory impulses that are transmitted from one muscle to the spinal cord, thus causing reflex muscle contraction. The contraction itself stimulates the same sensory receptors even further causing the spinal cord to increase the intensity of the contraction further. Thus a positive feedback mechanism occurs so that a small amount of initial irritation leads to more & more contraction until the muscle goes into a cramp like spasm.
Reciprocal inhibition can sometimes relieve the cramp.
As Osteopathic practitioners we cannot view the symptoms of pain and restriction in isolation. If inadequate attention is paid to the degree of acuteness or chronicity their relationship with the whole body and its systems (including the emotional & nutritional status of the individual plus their environmental, occupational, social and other factors that may impinge upon them) then it is quite possible that they will receive inappropriate treatment. A patient with major social, economic and emotional stressors present in their life arrive for treatment to a muscular pain and backache is unlikely to respond other than in the short term, to manual techniques if we ignore the enormous multiple coping strain we are handling. Therefore it is important to understand the process by which stress and secondary stress influence muscles.
- Stress causes biomechanical changes in the brain partly involving neurotransmitter production, which increases neural excitability;
- Postural changes occur in muscles in muscles that have increased tone, which inhibits local circulation causing a build-up of calcium, lactic acid and hyaluronic acid;
- Local contractile activity in muscle is because of the interaction between calcium and adenosine triphosphate (ATP) leading to physiological contractions that shorten and tense muscle tissue.
- Sustained metabolic activity in such muscles increases neural hyper-activity that may stimulate reflex vasoconstriction leading to local tenderness and pain.
- Relative oxygen lack and reduced energy supply results from decreased blood flow leading to ischaemia. Pain is a feature of this process due to accumulation locally of chemicals lactic acid inflammatory exudates histamine. Local pressure build up involving these chemicals and local metabolic wastes and/or local ischaemia are sufficient causes to produce pain and local muscle spasm.
Stressor Factors Leading to Musculoskeletal Dysfunction
- Acquired postural imbalances
- Use related stress; occupational/recreational.
- Developmental imbalance; short leg/arm, hemivertebrae, fascial distortion.
- Functional imbalance; pelvic torsion, pes planus, functional scoliosis.
- Repetitive strain; occupation, hobby, sport.
- Emotional stress; bereavement, familial, work.
- Trauma leading to inflammation and fibrosis within the muscle.
- Disuse/immobilisation i.e. following a fracture/frozen shoulder.
- Reflex related; viscerosomatic, myofascial.
- Weather related stress; severe chilling, fear of tsunami, tornado etc.
- Nutritional imbalance; lack of vit C reduces collagen efficiency.
Stressor Factors Cumulatively Demand Increased Muscular Tone Causing the Following Events
- The muscles antagonistic to the hypertonic group become weaker as may the hypertonic group themselves. The hypertonic stressed muscles develop areas of hypoxia and ultimately ischaemia resulting in the build-up of metabolic waste products;
- This toxic build up and oxygen lack leads to irritation, sensitivity pain and at times oedema. If inflammation is part of the process fibro tic changes in connective tissue tend to follow. Neural structures in the area also become facilitated & hyper-reactive to stimuli adding to the imbalance & dysfunction of the area;
- The tendinous insertions of the hypertonic muscles become stressed and painful leading to tendonitis & eventually periostitis. (esp. noted in golfers & tennis elbow). If any of the hypertonic tissues cross-joints a degree of imbalance occurs (agonist & synergist, one being hyper whilst the other is hypotonic) and abnormal movement patterns evolve, resulting in joint dysfunction;
- Localised active trigger points will also occur in in highly stressed/ischaemic tissue and will become responsible for the development of new dysfunction in distant target tissue typically inhibiting antagonistic muscles. This is further exacerbated by energy wastage leading to fatigue in local tissue and generally, which if it involves respiration will lead to an impact on vital function;
- Over time the CNS learns to accept altered patterns of use as normal, adding further to the complication of recovery since rehabilitation will now demand a relearning process as well as the structural shortening & functional weakness corrections.
History and Development of MET
Muscle energy technique is an osteopathic technique that goes back to AT Still. Still did not record the way he treated. He preferred that his students learnt anatomy and osteopathic philosophy so as to work out treatment plans and develop their own technique. This is what Dr F Mitchell DO did by developing a plan of diagnosis & treatment that he called Muscle Energy, which relies on active patient participation through muscular contraction. This technique is used to increase joint movement, lengthen muscle fibres and even increase muscle tone and increase local circulation.
This technique requires active patient participation therefore it cannot be used if the patient is uncooperative, unresponsive or has a poor command of English and does not understand your commands.

Muscle Energy Technique MET Tensor Fascia Latae (TFL)
MET can be divided into 3 groups:
ISO-Tonic: Patient wins increasing muscle tone (weight lifting)
ISO-Metric: Equal & opposite force, stretch after contracture reduces tone. Also used to Increase joint movement.
ISO-Lytic: Operator wins’ forcibly stretching contracting muscle reduces tone.
MET Basic Physiological Principles
Iso-metric/Iso-lytic Techniques; Following an iso-metric contracture the muscle spindle/ golgi tendon apparatus(neuro-muscular apparatus) is in a refractory state during which strong passive stretching can be performed. The brain interprets this data as lengthened muscle fibres and thus fires off fewer gamma efferent impulses (turning down gamma gain). This results in the target muscle remaining in a more lengthened state.
With iso-lytic techniques the operator overcomes the patients contracture, forcibly stretching muscle fibres and hence the neuro-muscular apparatus. Again the brain interprets this data as lengthened muscle fibres and fires off fewer gamma efferents. Hence muscle tissue remains in a more lengthened state.
Activating Forces
- These are needed to make techniques work and are divided into 2 groups.
- Extrinsic forces come from outside the patient i.e. effort exerted by the operator carrying out an HVT or traction;
- Intrinsic forces come from within the patient i.e. active muscle contraction exerted by the patient in MET;
- In MET the operator offers a stabilizing force (effectively creating a false origin) as the patient uses active muscle force. The operator usually positions the patient’s tissues at the initial point of resistance to a specific movement and then offers resistance or counterforce to the patient’s contracting target muscle. Thus MET is carried out within a range of movement against a sense of increased tension/resistance.

Energy Technique (MET) Piriformis
Carrying Out Muscle Energy Technique (MET)
Diagnosis
Usually used on patients with hypertonic/fibrotic muscle tissue, preparation prior to an HVT or as an alternative to increasing joint range of motion.
Procedure
- The operator positions the joint or body part/muscle group in the appropriate position of initial resistance;
- The operator instructs the patient about his /her participation;
- The operator directs the patient to contract the appropriate muscle/group;
- The operator uses counterforce in opposition to and equal to the patient’s muscle contraction or overcomes it if carrying out iso-lytic stretch;
- The operator maintains forces until an appropriate patient contraction is perceived at the target joint or muscle, which should last for between 3 & 5 seconds;
- The patient is instructed to gradually cease contraction while the operator matches this with a gradual decrease in counterforce;
- As the patient relaxes the operator senses proprioceptively the change in tissue tone/joint motion;
- The operator takes up the slack created by the decreased muscle tone or increased joint motion. The slack is allowed by reduced tension in the tight muscle, allowing it to be passively lengthened, whereby the operator should note an increased range of movement;
- Steps one to eight are repeated two to five times until the best possible increase in movement and reduced muscle tone is obtained, the quality of response often peaks after three, with diminishing returns thereafter;
- Re-check muscle tone & range of motion.
Contraindications
MET should not be used in the following; muscle tear, haematoma, DVT, post-surgery and patient’s with low vitality
Comments:
-
No Article Comments available