Positive Health Online
Your Country

![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Lotus Books]](/img/original/TopicbannerAvatar/953.adb373b0210368e0c9ce4d9a8a9f01aa.jpg "Lotus Books")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
LEAP for the Assessment and Correction of Specific Learning Difficulties
by Susan J McCrossin(more info)
listed in kinesiology, originally published in issue 50 - March 2000
In the last few decades, scientific research has continued to develop insights into understanding the complex functions and capabilities of the human brain that amaze and astound us, while reminding us of just how little in fact we know. Concurrently, kinesiology, or muscle testing, has developed at a similar rate since it was first developed by a Boston orthopaedic surgeon, RW Lovett, in 1932.[1] Our own research and clinical experience since 1988 has evolved to an understanding of brain function that has just recently been supported by scientific research.[2] The techniques we have developed are now available in a protocol we call LEAP, the Learning Enhancement Advanced Programme. This approach can be very effectively applied to specific learning difficulties in children and adults with consistent success, where previously medication was the most common intervention with very limited success.[3]
LEAP helps all kinds of learning difficulties for children as well as adults such as: attention deficit disorder (ADD) both with and without hyperactivity, sensory integration, dyslexia, poor co-ordination, closed head traumas, brain injuries, autism and nervous breakdowns. It enhances learning abilities and improves reading, reading comprehension, spelling and co-ordination.
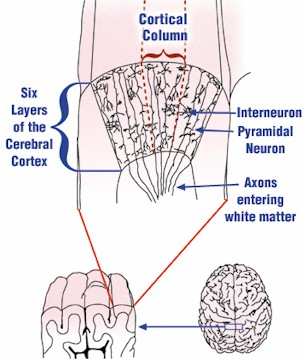
Figure 3 (above): Cortical Columns. Vertical slabs of cortex consisting of all six distinct cell layers, called cortical columns, are the functional units of the cerebral cortex. Some of the cells like the large pyramidal cells have dendrites that extend through almost all layers and axons that exit the grey matter to become part of the white matter tracts carrying information to other parts of the brain and body. There are also innumerable interneurones connecting the cells within each cell layer and between the layers.
History of LEAP: The Evolution of a New Kinesiological Paradigm
During the late 1980s, kinesiology, as it was then practised, allowed access to brain structures only in a very general way. We could detect that there were stresses related to specific learning processes, but did not understand how to go beyond this first step to tap into the hierarchical processing of the brain to determine which specific brain functions might have gone off-line. What had become clear to us was that the brain processed in a modular fashion, with single functions antecedent to many other functions. If one of these antecedent functions was compromised, all of the processes dependent on this function would also show deficits. We had to find a way to get into these processing modules.Just as these problems were arising for us, synchronicity stepped in with a solution. In 1989 Richard Utt, at his International Institute of Applied Physiology, developed new techniques of brain physiology formatting that added to the existing model of kinesiology by focusing on the physiology of the brain itself. He did this by applying understandings from the 5000-year-old Chinese acupressure system to his working understanding of brain function.[4]
With Utt’s brain physiology formatting we had the map of the primary neurological processing modules and a basic format with which to access them. Now we had a way in and from there on it was a matter of asking the right questions of the right structures. Then, for instance, we could ask the brain if there was any stress in the posterior hypothalamic nuclei. If stress was present as indicated by muscle response, we could then proceed to determine if there was stress in the part of the posterior hypothalamic function that controlled dilation of the pupils in relation to the fight or flight response.
Once the stress had been identified, the factors causing that stress could be pinpointed. Knowing what those stresses were, we could then apply kinesiological and acupressure techniques to resolve them. As soon as the stress, or stresses that have caused the block or shutdown of functions are resolved, these processes so vital to learning come back on-line.
We began to obtain much better results and 90 per cent of our clients started showing positive changes, yet perplexingly, there still remained a recalcitrant group that eluded our methods. What was it that we did not yet understand? To find out, we sent these children for assessment by a neurologist who specialised in epilepsy and learning problems. Using magnetic resonance imaging (MRI) and other assessment techniques, it was revealed that in all but one of the cases, the underlying cause was organic brain damage.[5] Their problem was more than a glitch in the software. The hardware itself had been damaged.
Frequency of Specific Learning Difficulties
Frequently, children who are diagnosed as learning disabled are also inattentive and deficient in linguistic skills, most often in reading.6 Estimates of the prevalence of learning disorders in broad age ranges7,8 is problematic because a learning disability is an emergent problem that is often not evident until later years in schooling. Using the criterion of defining learning disorders as being two years behind on standardised tests, less than 1% of 6-year-olds are disabled, 2% of 7-year-olds and so on until at age 19, 25% would be classified as learning disabled. These children fall progressively behind as they mature and the complexity of work increases.9 In an address given by the Australian Federal Schools Minister, Dr David Kemp, in October 1996, Kemp stated that a study of 28,000 students in four surveys in Australia found that 30% of year 9 students lacked basic literacy skills. This high incidence of learning disorders in school children indicates a need for effective treatment.Causes of Specific Learning Difficulties
Currently, the possible causes of learning disorders are believed to be primarily the result of five major factors: - structural damage;
- brain dysfunction;
- abnormal cerebral lateralisation;
- maturational lag; and
- environment deprivation. While none of these theories is unequivocally supported by current data, all of these factors may contribute to learning disabilities.[10]
This is supported by studies of children with learning disorders which show that they have difficulty on continuous performance tests requiring attention and low distractibility; had slower reaction times to stimuli, and increased errors due to impulsivity on tests of visual searching.[15] Douglas proposed that the deficits on these tasks resulted from inadequate cerebral activation. Learning disorders of some types at least, do improve with drugs like amphetamines that cause cerebral activation via increasing subcortical arousal. In fact, this is the basis of treating hyperactive children with Ritalin,[16] although it is not an approach that treats the cause of the problem, nor is there evidence that it improves academic performance.[17]
An alternative model of learning disorders is based on recent neuro-physiological findings which suggest it is the timing and synchronisation of neural activity in separate brain areas that creates high order cognitive functions. Any loss or malfunction of the timing mechanism may cause the disintegration of neural activity and hence dysfunction in cognitive tasks.[18] If the brain does integrate separate processes into meaningful combinations that we call ‘thought’ or cognitive ability, then the main risk is mis-timing or loss of synchronisation between these processes, which could result in learning difficulties. Antonio Damasio, a leading American neurologist states that “any malfunction of the timing mechanism would be likely to create spurious integration or disintegration”.[19]
This model supports the approach (LEAP) that Charles Krebs Ph.D. and I have been developing since 1988.[20] In our LEAP model, learning disorders are based on the disruption or loss of timing and synchronisation between the neural activity in the diverse brain regions, both cortical and subcortical, that must be synchronised in order for successful integration to produce normal cognitive activity. Our clinical experience with thousands of cases indicates that learning difficulties arise from a lack of integration of functions that should occur simultaneously in separate brain regions.
Models of Learning Based on Gestalt and Logic
For the past 20 years or so the Right Brain-Left Brain model of learning has popularised the notion of ‘right brain’ designating the right cerebral cortex having Gestalt functions and ‘left brain’ referring to the left cerebral cortex having Logic functions.[21]While Gestalt functions do appear to predominate in the right hemisphere and Logic functions appear to dominate in the left hemisphere, we argue that this model oversimplifies to an enormous degree the complexity of the many cortical subsystems – many of which are located in both cerebral hemispheres. Recent scanning techniques support this and reveal that women are less lateralised in brain function than men in many areas. Further, the prevailing theory totally ignores the subcortical processes that are, in fact, major centres of our mental processing. It is the subconscious that does most of the actual processing, but it is the conscious areas of the cortex that direct what is processed.
It is a controversial view because we believe that a specific hemisphere does not entirely dominate either Gestalt or Logic processing. Rather, they provide the lead, or the conscious intent that activates a number of other cortical and subcortical areas to perform the essential processing.
The actual processing units of the cerebral cortex are called Cortical Columns. Newer research has shown that these vertical columns bisect all six layers, forming distinct processing units. Cortical Columns are not circular columns in the architectural sense; rather, they are long, three-dimensional slabs up to 0.5 mm wide and variable in length[22] (see Fig. 3). Each cortical column is concerned with a specific type of function, and as functions vary in complexity so the columns vary in size. Sometimes, several columns may be involved in performing a single more complex function. Along the sensory cortex, each column is concerned with sensory input from a particular region of the body.[23]
Since the cortical columns are the processing modules that relate to specific types of cortical function, they are the centres for the Gestalt and Logic lead functions. These lead functions provide a point of entry into an inter-linked set of cortical and subcortical modules, which includes the corpus callosum, and performs our mental functions.
When you read words on a page, cortical columns that perform various Gestalt lead functions involved with the decoding of symbols will be activated by the visual stimulus of those words. This will in turn activate other cortical columns, housing Logic lead functions involved in understanding the meaning of words and their grammatical relationships.
An analogy of this process is what happens when you decide to turn on a light. This is a conscious mental decision. As soon as you flick the switch, a whole cascade of other events occur. Electrons begin to flow invisibly through wires, junction boxes, the light fixture itself and into the bulb. All of this occurs outside of your conscious awareness. All you are aware of is that the light has come on. This is an electrical model, but it is very similar to what happens in the brain. In the brain, you make a conscious request to do something – whether mental or physical – and this conscious input from a particular cortical lead function creates a subconscious flow that results in the processing of that request. The end result is conscious awareness of the outcome.
The essential point of the theory is that the conscious cortical lead functions in each hemisphere merely provide the entry point. The cortex can only provide a lead if the point of entry is intact or accessible.
Brain integration is the dynamic synchronisation of the timing of neural and mental events. Any loss of synchronisation represents a loss of integration. Loss of integration in turn, results in loss of some specific mental capacity.[24,25]
Ideally, the brain is set up so that all areas of Gestalt and Logic processing are accessible and all the integration routes that connect them are totally clear. With this perfect set-up, all types of learning will be easy. Any blocks will make the process less efficient and more stressful with long-term effects on self-esteem and confidence for future learning experiences.
LEAP: Its Role in Correcting Specific Learning Difficulties
From this model, our clinical experience shows that if any specific subconscious function is ‘blocked’ for any reason, then the mental processes dependent upon that function are compromised or often cannot be performed at all.Learning problems then result, either from ‘blocked’ access to one or more subconscious functions, or from a ‘block’ preventing integration of the functions accessed. In more severe learning difficulties there may be both ‘blocks’ to specific functions and ‘blocked’ routes of integration, which makes it doubly difficult for people to overcome learning problems of this nature.
Kinesiology not only provides a means of identifying where these ‘blocks’ in function occur, as noted above, but more importantly, provides a means of identifying the nature of the disturbance causing the ‘block’ in function. Muscle monitoring provides an interface between neurological function and the more subtle energies of the energetic, emotional and mental bodies.[26,27]
LEAP provides a coherent protocol for the correction of most specific learning difficulties (SLDs). This protocol was established over several years based on the hierarchical processing in the brain. Perhaps to conserve space and yet provide for a variety of functions, the brain functions are not organised in a hierarchical fashion with a linear flow of neural impulses; rather the neural flow is parallel and multiplex, including transfer of information that does not even flow along nerves. In this multiplex, parallel processing many of the central basal subconscious brain functions are used in many different types of processing, as a central processing unit capable of multi-tasking. Thus, this central processing unit of subconscious brain functions when not being used in one type of function may be used in another, or may even carry out several types of function in parallel.
When the functions of reading or spelling, or any learning task, cannot be performed properly, it is usually not in the cortical lead functions that the problems lie. The person most likely understood the command to read or spell and via their cortical lead function asked the brain to perform this function. Rather, the problem is usually ‘blocks’ in or to their subconscious processing centres that are required to perform the requested task. Since most learning problems result from a lack of access to specific subconscious functions, clearing the blocks to these functions will rectify the learning problems. However, there is a specific order in which the basal subconscious functions must be ‘cleared’ to produce consistent results, and these are related to the hierarchy of sensory information processing in the brain. The LEAP protocol follows this hierarchy, locating and treating the exact subconscious function that is blocked and thus providing consistent, long-term results in the treatment of SLDs.
Brain integration can also be very fragile, in the sense that it is largely determined by one’s stress levels. Even the most well-integrated person, given enough stress of a specific type, will lose integration and become temporarily dysfunctional. One of the major differences between people is the type of stress and the extent of stress required to cause loss of brain integration.
Leap in Application
In a given session the electro-magnetic activity in the brain is assessed using muscle testing and acupressure. The correction technique could involve any one of a number of kinesiological techniques to re-establish electro-magnetic integrity within the brain. Thus, brain functioning is improved.A way of exemplifying the power and effectiveness of the LEAP programme is to look at some of the cases to which it has been applied. The following few cases illustrate the typical responses we see with people treated with the LEAP protocol.
Sharon’s Story
When we first saw Sharon she was 15 and presented as being very Gestalt dominant, which is by far the most common outcome of corpus callosum shutdown. In our assessment protocols, Sharon demonstrated very poor access to Logic function. She was attractive, charming and very witty, which is the way many Gestalt dominant people compensate for their high level of Logic dysfunctions. Everyone likes a charmer and will usually help them because they are so delightful to have around. Sharon was progressing through school with her classmates but was consistently failing in maths.In year 10, she could not add up numbers greater than 10. She did not know how to carry a digit and couldn’t add, subtract, or do fractions. At 15, she could not abstract arithmetical concepts that a primary school student could manage easily, yet was so personable and popular that she had been promoted through the grades with her peers.
After about 10 hours of treatment, to complete the whole LEAP protocol, we addressed her presenting problem, which was her difficulty with maths.
We showed her the process of adding and carrying numbers, a technique she had probably been shown hundreds of times before. She suddenly said: “Oh, that’s how you do it!” With her new access to Logic available, she could instantly grasp the concepts. We gave her harder problems, and she easily generalised what we were teaching her, and could now deal with elementary arithmetic.
Our job is not to tutor students, so having opened up her functions, we sent her to a maths tutor for remedial work. In the five weeks of her summer holidays she was able to come up to the maths levels of her classmates. She went from basic numeracy all the way to algebra. Her tutor told us that in 25 years of tutoring students she had never before seen anyone make such rapid progress. Sharon’s reading and comprehension also improved, as did her spelling. Her self-esteem rose alongside her performance. This is an example of how devastating SLDs can be on one’s self-esteem.
Maxine’s Story
Maxine is an adult who had been a gifted learner until a car accident a few years ago. She had a “low-impact, closed head injury” and consequently could not even put a shopping list together. She is now at college completing a degree.Trevor’s Story
Trevor came when he was 14 years old with strong Gestalt dominance. His inability to read had led him to decide to drop out of school. After the treatment, reading became easy and enjoyable, he completed high school and went on to study photography. His work was so outstanding that he has received the only Certificate of Merit awarded by his faculty for his innovative work in professional film developing. He has a job advising photographers on their equipment and designing new equipment for them and his employer has offered to pay for him to further his studies into electronics.Further information
For a full discussion of kinesiology and muscle testing you are referred to Dr Krebs’ new book, A Revolutionary Way of Thinking. Hill of Content Publishing. Melbourne. Australia.References
1. Krebs CT and Brown J. A Revolutionary Way of Thinking. From a Near Fatal Accident to a New Science of Healing. Hill of Content Publishing. Melbourne. p40. 1998.2. McCrone J. Left Brain Right Brain. New Scientist. 3 July 1999.
3. Krebs CT and McCrossin SJ. Learning Enhancement Advanced Program (LEAP). Melbourne Applied Physiology. Melbourne. 1994.
4. Utt R. Applied Physiology Acupressure Formatting for Brain Physiology. Applied Physiology Publishing. Tucson, Arizona. 1991.
5. Jackson G. Personal Communication, June 1990 – July 1992.
6. Aiken LR. Assessment of Intellectual Functioning. 2nd ed. Plenum Press. New York. 1996.
7. Rutter M and Yule W. The concept of specific reading retardation. J. Child Psych & Psychiatry. 16: 181-197. 1975.
8. Gaddes WH. Prevalence estimates and the need for definition of learning disabilities. in Knights RM & DJ eds. The Neuropsychology of Learning Disorders. University Park Press. Baltimore. 1976.
9. Kolb B and Whishaw IQ. Fundamentals of Human Neuropsychology. 3rd ed. 1990.
10. Kolb B and Whishaw IQ. ibid.
11. Kolb B and Whishaw IQ. ibid.
12. Hughes JR. Electroencephalographic and neurophysiological studies in dyslexia. in Benton AK and Pearl D eds. Dyslexia: An appraisal of Current Knowledge. Oxford University Press. New York. 1978.
13. Farrow M et al. Prefrontal & parietal deficits in ADHD suggested by Brain Electrical Activity during Children performing the AX-CPT. Ed. Develp. Psych. 13: 59-68. 1996.
14. Kolb B and Whishaw IQ. Fundamentals of Human Neuropsychology. 3rd ed. 1990.
15. Douglas VI. Perceptual and cognitive factors as determinants of learning disabilities: A review chapter with special emphasis on attentional factors. in Knights RM & DJ eds. The Neuropsychology of Learning Disorders. University Park Press. Baltimore. 1976.
16. Serfontein G. The Hidden Handicap. Simon & Schuster. Sydney. 1990.
17. Krebs CT and McCrossin SJ. Learning Enhancement Advanced Program (LEAP). Melbourne Applied Physiology. Melbourne. 1994.
18. Damasio AR. Descartes’ Error: Emotion, Reason and the Human Brain. Grosset/Putnam. New York. 1994. Nunez. PL. Neocortical Dynamics and Human EEG Rhythms. Oxford University Press. New York. 1995.
19. Damasio AR. Descartes’ Error: Emotion, Reason and the Human Brain. Grosset/Putnam. New York. p94. 1994.
20. Krebs CT and McCrossin SJ. Learning Enhancement Advanced Program (LEAP). Melbourne Applied Physiology. Melbourne. 1994.
21. Parker A and Cutler-Stuart J. Switch on Your Brain. Hale & Ironmonger. Petersham, NSW. 1986.
Springer SP and Deutsch G. Left Brain Right Brain. 3rd ed. W.H. Freeman & Co. New York. 1989.
Dennison P. and Dennison GE. Brain Gym. Teachers Edition, Revised. Edu-Kinesthetics, Inc. 1994.
Hannaford C. Smart Moves. Great Ocean Publishing Inc. Arlington, VA. pp177-197. 1995.
22. Noback CR, Strominger NL. and Demarest RJ. The Human Nervous System. 4th ed. Lea & Febiger. London. pp398-401. 1991.
23. Kolb B and Whishaw IQ. Fundamentals of Human Neuropsychology. 3rd ed. pp185-189. 1990.
24. Damasio AR. Descartes’ Error: Emotion, Reason and the Human Brain. Grosset/Putnam. New York. pp84-113. 1994.
25. Damasio AR. Ibid. pp84-164. 1994.
26. Krebs CT and Brown J. A Revolutionary Way of Thinking, From a Near Fatal Accident to a New Science of Healing. Hill of Content Publishing. Melbourne. 1998.
27. Levy SL and Lehr C. Your Body Can Talk. The Art and Application of Clinical Kinesiology. Hohm Press. Prescott, Az. pp4-5. 1996.
Comments:
-
No Article Comments available