Positive Health Online
Your Country

![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Human Kinetics Trail Guide to the Body]](/img/original/TopicbannerAvatar/4656.d9ccc329faa3d1500b4807b369feccef.jpg "Human Kinetics Trail Guide to the Body")
![[Image: Lotus Books]](/img/original/TopicbannerAvatar/953.adb373b0210368e0c9ce4d9a8a9f01aa.jpg "Lotus Books")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
Myofascial Trigger Points and Beyond
by Simeon Niel-Asher(more info)
listed in bodywork, originally published in issue 121 - March 2006
What is a trigger point?
Have you ever felt tight little lumps in muscles you have been massaging? Often these can range in size from a 'tiny lump' to 'little peas' to 'large lumps'; they can be felt beneath the surface embedded within the muscle fibres. If they are tender to pressure they may well be 'trigger points'. So tender in fact that when they are pressed, the patient often winces from the pain; this has been called the 'jump sign'.[1]
Defining the trigger point
The trigger point can be defined as "a highly irritable localized spot of exquisite tenderness in a nodule in a palpable taught band of (skeletal) muscle." (Travell & Simons. 1993)[2] which when stimulated causes a specific referred pattern of pain. (See Figure 1).
Figure 1: A trigger point (*the blue symbol indicates the location of a trigger point).

Figure 2: Pectoralis major – Trigger Points and Referred Pain Patterns.
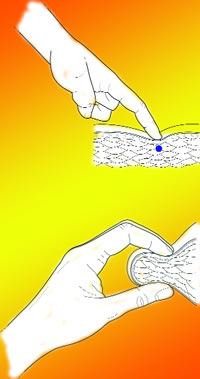
Figure 5. Reciprocal Inhibition Technique. Cortico-neuro-somatic-programming (CNSP)
Referred Pain Patterns
Pain is a complex symptom experienced differently and individually. However, referred pain is the defining symptom of a myofascial trigger point.
You may be used to the idea of referred pain of a visceral origin; an example of this is heart pain.
A myocardial infarct (heart attack) is often not experienced as crushing chest pain, but as pain in the left arm and hand, and the left jaw. This type of pain is well-documented and known to originate from the embryological dermomyotome; in this case, the heart tissue, jaw tissue, and arm tissues all develop from the same dermomyotome.
Referred pain from a myofascial trigger point is somewhat different. It is a distinct and discreet pattern or map of pain. This map is consistent and has no racial or gender differences. The pain is generated by stimulating an 'active' trigger point.
Patients describe referred pain in this map as having a deep, aching quality; movement may sometimes exacerbate symptoms making the pain sharper. An example of this might be pectoralis major muscle (See Figure 2); stimulating the trigger points embedded in the myofascia leads to a distinct 'pattern' or map of pain. Symptoms in the pectoralis major may arise for a variety of reasons, for example:
| • Cardiac arrhythmia; • Post myocardial infarction; • Mid scapular back pain; • Prolonged rib/breathing dysfunction; • Breast pain, mastitis, hypersensitivity; • Thoracic outlet syndrome; • Anterior shoulder pain; • Golfers/tennis elbow; • Other. |
How do trigger points develop?
Trigger points develop within muscle sarcomeres. Sarcomeres are the basic building blocks of muscles consisting of actin and myosin myofilaments; muscles move when these myofilaments slide over one another (See Figure 3). When we move, the brain sends signals via the motor nerves to switch on and off millions of sarcomeres in co-ordinated sequences. Trigger points develop when this process becomes attenuated and the sarcomeres becomes overactive; the actin and myosin myofilaments stop sliding over one another. As a result, the sarcomere becomes turned to the permanently 'switched-on' position leading to a state of contraction. We are still not 100% sure what causes this to happen, but it is probably multifactorial.
If this situation is allowed to persist over a significant period of time, the above changes lead to a vicious cycle. Calcium is unable to be taken into the actin and myosin myofilaments leading to sarcomere 'failure'.
Over time this situation may become chronic. Eventually the brain sends a signal to rest the muscle in which the trigger point manifests. This leads to muscle hypertonia, weakness, shortening, and fibrosis (muscle stiffness). Treatment is thus aimed at interfering and disrupting this vicious cycle.
Classification
Trigger points are described in various ways according to their location, tenderness and chronicity: central (or primary); satellite (or secondary); attachment; diffuse; inactive (or latent); and active. (see box below)
|
Trigger Point Classification Central (or Primary) Trigger Points Satellite (or Secondary) Trigger Points Diffuse Trigger Points Active Trigger Points |
Treating the trigger point
A number of therapeutic interventions are available to the therapist; the good news is that many of these are not difficult to learn and are extremely effective in reducing symptoms. The most common treatment approaches include:
Injections/wet needling
This technique can have a rapid and profound effect in 'switching off' a trigger point. Substrates include for example; procaine hydrochloride 1% solution and/or Lidocaine hydrochloride (0.5%).
Dry Needling Technique
This is almost as effective as wet needling; here acupuncture needles are inserted into the trigger point.
Spray and Stretch Technique
Again, this technique is quick and very effective, especially in large muscles with multiple trigger points such as the hamstrings. (See Figure 4).
Hands-on Therapy
These techniques are the most readily available to the manual therapist. Over time a number of effective techniques have been developed such as Reciprocal Inhibition (see Figure 5), Muscle Energy Techniques and/or Stretch and Release; each has its own place in management: Massage Techniques include Inhibition – Ischaemic Compression Technique and/or Deep Stroking Massage Technique.
As an Osteopath, I blend the treatment of trigger points with osteopathic manipulation and other soft tissue techniques. I have found it a quick, efficient and an effective way of managing the soft tissue component of somatic dysfunction.
In 1997 by chance, I began to see a group of patients with a similar pattern of soft tissue dysfunction; these patients' all had 'adhesive capsulitis' (frozen shoulder syndrome). This is an enigmatic condition which, until now, has been poorly understood and even more poorly managed. Over time, I have developed a robust method of treatment for capsulitis and a range of other complex shoulder problems. This technique significantly (and dramatically) improves the range of motion, strength and power, whilst reducing pain.[3]
The manipulation of specific trigger points is a key component within my approach; however, sequencing the release of trigger points is the key. Trigger points develop in the shoulder muscle agonist, antagonist and fixators. I literally utilize these somatic reflexes (including the pain reflexes) to re-programme the way the brain (somato-sensory) senses itself and thereby – re co-ordinates (somato-motor) movement.
Maps
We are born with two 3-dimensional images of our body hard-wired, in our (somato-sensory and somato-motor) cerebral cortex. The sensory map receives a constant flow of feedback from a plethora of sensors embedded in our tissues especially in the skeletal muscles. Our physical 'image' of self is constantly being re-enforced via these sensors. Our brain however, does not see us in the same way we see ourselves; it sees us as a homunculus (see Figure 6).
As can be seen, certain regions of the body have a disproportionate representation; especially the shoulder which is relatively poorly represented. Movement is co-ordinated in the somato-motor cortex and manifest via sequential stimulation of millions of sarcomeres at any one time. In a frozen shoulder the feedback from the skeletal muscles becomes deranged; furthermore the motor cortex and local spinal reflexes establish an antalgic muscular pattern of shoulder joint restriction (the capsular pattern). Various sarcomeres are forced into the permanently 'switched on' position, and trigger points develop in a specific (and reproducible) pattern. Muscles become hypertonic, weak, shortened, and fibrotic. Without treatment, this situation persists for an average of 30 months (and maybe longer).[4]
The Niel-Asher Technique
The Niel-Asher Technique utilizes a specific sequence of manipulations to the shoulder joint and its soft-tissues. The technique is basically the same each session; each treatment session reinforcing the previous treatment. Treatment stimulates a specific neurological profile at both the somato-sensory cortex (map) and local spinal reflex levels in the cord. The longer a patient has been suffering, the quicker the results; the dramatic improvement in patient's symptoms can only be explained neurologically. I sequentially stimulate three trigger points (each) embedded in the agonist, antagonist and fixator. This also affords the sensory map an opportunity to re-orientate itself. I call this concept Cortico-Neuro-Somatic-Programming (CNSP). See Figure 5.
Unlocking the secrets of the frozen shoulder has led me to a deeper understanding of how to release somatic dysfunction quickly, effectively and reproducibly. The theory underpinning my technique may have wider implications.
References:
1. Travell, J & Simons, D. Myofascial pain and dysfunction: The Trigger Point Manual. (vol. 2). Lippincott, Williams and Wilkins, Baltimore. 1993.
2. Ibid.
3. JT Wies, S Niel Asher et al. A pilot randomised placebo controlled trial of physiotherapy and osteopathic treatment for frozen shoulder. British J Rheumatology, Volume 42. Supplement 1. BHPR 418. 2003.
4. Baslund B: Frozen shoulder current concepts. Scandinavian J Rheumatology. 19: 321-325, 1990.
Comments:
-
No Article Comments available