Positive Health Online
Your Country

![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
Clinical Impovements in CFS/ME: The Role of Fatty Acids
by Professor Basant K Puri(more info)
listed in cfs me long covid, originally published in issue 117 - November 2005
Chronic Fatigue Syndrome (CFS) or Myalgic Encephalomyelitis (ME) is a disorder affecting multiple body systems. When defined rigorously for research purposes, according to the revised criteria of the Centres for Disease Control and Prevention in Atlanta, it has been estimated to affect around three per cent of the general population.[1] These revised diagnostic criteria[2] are as follows:
1. Exclude any other cause for chronic fatigue;
2. Self-reported persistent or relapsing fatigue for six or more consecutive months;
3. Four or more of the following symptoms are concurrently present for over six months:
i. Impaired memory or concentration;
ii. Sore throat;
iii. Tender cervical (neck) or axillary (armpit) lymph nodes;
iv. Muscle pain;
v. Multi-joint pain;
vi. New headaches;
vii. Unrefreshing sleep;
viii. Post-exertion malaise.
As most practitioners of Complementary and Alternative Medicine will be aware, symptoms such as long-term fatigue and unrefreshing sleep are very common. Fortunately, the purely natural treatment with fatty acids (pure EPA and virgin Evening Primrose Oil) advocated in this article also gives excellent results in cases of chronic fatigue or unrefreshing sleep that do not meet rigorous research diagnostic criteria.
In the first section of this article, I shall explain why I believe that CFS has an infectious cause. This is important because it means that it is a physical illness rather than being, as some of my colleagues in the medical profession still advocate, a 'psychosomatic disorder'. The next section then details certain important aspects relating to long-chain polyunsaturated fatty acids of the Omega-3 and Omega-6 groups, and, in particular, why they can be used to treat CFS. Finally, specific details about prescribing fatty acids are given for Complementary and Alternative Medicine practitioners.
The Cause of CFS
Five converging strands of evidence now point to the main cause of CFS as being infectious in nature. I believe that the infectious agent is probably viral.
The first strand of evidence is derived from a consideration of some of the major outbreaks of this illness (albeit under different names in the past). A detailed examination of the illnesses suffered by those who were afflicted by the Los Angeles County Hospital epidemic of 1934 and the Royal Free Hospital epidemic of 1955 strongly points to an infectious agent. There appeared to be person-to-person contact between those affected, who all tended to be medical and paramedical staff. (To this day, I am told by one of my patients that there is a victim of the Royal Free outbreak who is still suffering from CFS; she was working as a radiographer at the Royal Free Hospital in 1955.) In my clinical practice, it is also the case that there tends to be a common occurrence of a history of a viral-like illness just before the onset of CFS. Sometimes this is put down to having suffered from an episode of influenza. Some of the features of CFS, such as the chronic fatiguing illness itself and the muscle weakness, are known consequences of viral infections.
The second line of evidence is from studies of the immune system. Changes in particular types of white blood cell have been noted in well-conducted studies of CFS.[1] In summary, these are:
• Reduced NK cell (killer cell) activity;
• Reduced Th1 cell (helper cell type 1) activity;
• Increased Th2 cell (helper cell type 2) activity;
• Increased Tc cell (cytotoxic cell) activity.
If you are not familiar with killer, helper and cytotoxic cells, there is no need to worry. The important thing is that the changes described above are consistent with the immune system reacting to a pre-existing long-term viral infection.
The third strand of evidence comes from direct studies of blood levels of fatty acids in CFS patients. Professors Peter Behan, Wilhelmina Behan and David Horrobin published a key paper in 1990 showing that there were reduced levels of some long-chain fatty acids in the CFS patients they studied.[3] (In those days, the condition was also known as postviral fatigue syndrome.) A more recent study by Professor Malcolm Peet's group in Sheffield, published in 1999, found that CFS patients had a reduced level of the long-chain polyunsaturated Omega-3 fatty acid eicosapentaenoic acid, or EPA for short.[4] EPA is an extremely important fatty acid, and I shall have more to say about it later in this article. Meanwhile, suffice it to say that viral infections are one of the factors that can prevent the body from synthesizing its own long-chain polyunsaturated fatty acids from dietary short-chain precursors. So the blood results from these two studies are consistent with a viral infection in CFS.
The fourth line of evidence was first discovered at Hammersmith Hospital in London by my group.[5] By carrying out a specialized brain examination known as proton neurospectroscopy, using a magnetic resonance imaging scanner, we were able directly to examine the chemistry of the living brain in patients with CFS. We found strong evidence of a chemical signature in the patients which was consistent with an inability of the body to create the all-important phospholipid molecules (see the next section) in cell membranes in the brain. This could easily result from a lack of long-chain polyunsaturated fatty acids in the brain. In turn, this could be caused by a viral infection stopping the body from being able to manufacture these fatty acids. Our Hammersmith Hospital results were replicated by another group, working in Glasgow, under Professor (then Dr)Abhijit Chaudhuri, who also found evidence of the same chemical signature.[6]
Finally, just this year Dr Jonathan Kerr's group at Imperial College London reported the results of their work on gene expression in white blood cells (mononuclear cells) taken from patients with CFS.[7] Using a special microarray technique, which is rather like examining genes on a chip, Jonathan Kerr's group looked to see which, if any, of almost ten thousand human genes were expressed differently in 25 CFS patients compared with 25 age-, sex- and geographical location-matched normal controls. They found upregulation of the EIF4G1 gene in CFS. This is a fascinating finding which is consistent with the occurrence of a persistent viral infection in this disorder.
Fatty Acids
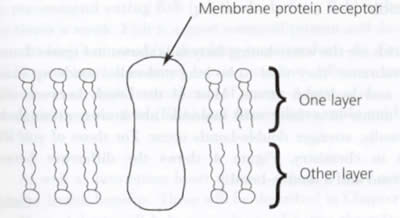
All human living cells have a boundary double-layered membrane. These membranes also surround certain organelles inside cells, such as the nucleus. The basic unit that makes up each layer is the phospholipid molecule. This consists of two water-hating fatty acids and a water-loving 'head' group. These are attached to a three-carbon glycerol backbone. Floating, as it were, within the double-layered membrane are membrane receptors. In order for these receptors to function properly, the phospholipid molecules must be properly constituted. In turn, this means that the right fatty acids should be present.
Figure 1(below) is a diagrammatic representation of a cell membrane, consisting of two layers of phospholipids and showing a membrane protein receptor.
In Figure 2 (below) you can see a summary of the way in which the body can make the certain important Omega-3 and Omega-6 long-chain fatty acids from the short-chain fatty acids linoleic acid and alpha-linolenic acid. Linoleic acid and alpha-linolenic acid are readily available from the diet. At each stage, as we go down the Omega-6 and Omega-3 pathways, an enzyme is needed. Only the enzyme for the first conversion (e.g. linoleic acid to GLA in the Omega-6 pathway) is shown in Figure 2. This is delta-6-desaturase.

The Omega-3 and Omega-6 fatty acids have very important roles in maintaining the correct structure of cell membranes. In particular, for a membrane to function properly, it needs to have sufficient levels of the Omega-6 long-chain polyunsaturated fatty acid arachidonic acid (AA), and the Omega-3 long-chain polyunsaturated fatty acid docosahexaenoic acid (DHA). Without these fatty acids, cell membranes become more rigid, and this reduced flexibility is reflected in poorer or abnormal functioning of receptors that lie in the membranes. In turn, this leads to impaired communication between cells, including brain cells.
An even more important role is that of the synthesis of eicosanoids in the body. These functions fall to two of the Omega-6 long-chain polyunsaturated fatty acids, dihomo-gamma-linolenic acid (DGLA) and arachidonic acid (AA), and one of the Omega-3 long-chain polyunsaturated fatty acids, namely eicosapentaenoic acid (EPA). Starting from dihomo-gamma-linolenic acid, arachidonic acid and EPA, the body can make all the families of prostaglandins, thromboxanes and leukotrienes (which collectively are eicosanoids). They are intimately involved in processes that are of the utmost importance in maintaining the health and wellbeing of the body and in fighting disease. These processes include:
• Blood clotting;
• Regulating the blood pressure;
• Reproduction;
• The response to disease or trauma (including inflammation responses, pain and fever);
• The secretion of acid by the stomach.
If the body has sufficient EPA, some of this can be converted into natural sleep mediators. This is one of the reasons why our patients (whether or not they had CFS to begin with) enjoy such wonderful, deep, refreshing sleep if they follow the advice to take a formulation each day that contains ultra-pure EPA (that is, EPA without any DHA) as mentioned in the last section below.
EPA is also important in helping the body to combat viral infections. It turns out that EPA can actually kill viruses in the body, without harming us in the process. It does this in at least two ways. First, EPA is itself directly viricidal. That is, if you add small amounts of EPA solution to harmful viruses (such as the Epstein Barr Virus that causes glandular fever), then the EPA actually kills the virus. Second, EPA is also indirectly viricidal. After being acted on by two sets of enzymes, EPA is converted into families of interferons, which, in turn, are powerfully antiviral.
Many viral species block the delta-6-desaturase enzyme. As you can see from Figure 2, this means that the body is no longer able to produce the long-chain Omega-3 and Omega-6 fatty acids. In the case of CFS, if I am right and there is a persistent (albeit perhaps low-grade) viral infection present, as suggested by the five strands of evidence detailed above, then there will be a long-term functional deficiency in these long-chain fatty acids. One result will be that there is insufficient EPA produced by the body to fight the viruses. There are other results too, as stated in my book1 on CFS:
Unable to make sufficient quantities of EPA, the human body is no longer able to manufacture sufficient quantities of the EPA-based natural sleep mediators. As a result, the body does not get enough deep refreshing sleep and ends up tired and even less able to resist the viruses. The lack of DGLA, arachidonic acid and EPA also means that the body cannot produce enough eicosanoids, and so the general health and wellbeing of the body suffers. The body cannot mount proper immune response measures against the invader, and has to endure long bouts of painful sore throats, and enlarged and tender neck (cervical) and armpit (axillary) lymph glands. EPA and certain eicosanoids normally help to keep our joints working properly and 'well-oiled'; their disappearance means that the body has to endure pains (arthralgia) in many different joints.
If these consequences were not bad enough, there is even worse to come. Blocking that first enzyme (delta-6-desaturase) also means that cell membranes cannot get enough arachidonic acid and docosahexaenoic acid so that they become more rigid and lose their normal flexibility. The effects on the protein receptor molecules that lie in the cell membranes are profound; the size and shape of these receptors change so that they no longer accept and pass on signals in the right way. Communication between cells is impaired. It would be like an enemy hitting our satellite and radar communications during a war. The results of this in the human brain are cognitive defects, such as problems with short-term memory and with concentration.
These results will sound familiar to any reader who is suffering from CFS. They constitute key symptoms and signs of this disease.
How to use Fatty Acids in Treatment
From what I have said so far, you might think that an effective way to treat CFS would be to by-pass the block at delta-6-desaturase by giving patients the long-chain Omega-3 and Omega-6 fatty acids directly. That is precisely what I do. There is evidence from two sets of studies that this approach works well[3][,][8] although one study was essentially negative.[4] Not only do the symptoms improve, but by giving EPA there is actually an improvement in the amount of brain tissue and its functioning.[9][,][10]
In terms of the fatty acids actually used by me, with good effect, I favour a combination of virgin evening primrose oil with ultra-pure EPA (that is, a DHA-free preparation).
The Evening Primrose Oil is a good source of GLA. From this fatty acid, the body's cells can easily biosynthesize dihomo-gamma-linolenic acid and arachidonic acid. By choosing the virgin (that is, cold-pressed, non-raffinated) form rather than ordinary (refined) Evening Primrose Oil, patients gain the added benefits of natural triterpines which act as free radical scavengers.[11]
On the EPA front, I definitely do not favour the use of ordinary fish oils at all for any of my patients. There are several reasons for this. I detailed these in my CFS book[1]:
Ordinary fish oil suffers from the same problems as the ones we have just mentioned: the risk from pollutants such as lead, mercury, cadmium, dioxins and PCBs. In fact, there are at least four reasons why the situation is even worse in respect of fish oil compared with just ordinary fish in the diet.
First, many of the harmful pollutants that are concentrated in the bodies of fish, such as dioxins and PCBs, are highly fat-soluble. This means that they are even more concentrated in fish oils (which, by definition, are oils and therefore fatty).
Second, we need to consider how fish oils tend to be extracted in industrial quantities from the bodies of fish. One method often used in industry is simply to squeeze the livers of the fish, and use (and sell) the liver oil thereby produced. A common example is cod liver oil, which has a good deal of EPA in it, and is extracted from the liver of cod. A major problem with this process is that in vertebrates such as fish (and, indeed, us), the liver is the main organ used for the detoxification of the blood. So, the liver oils can offer an even more concentrated concoction of dangerous pollutants. Another commonly used method is not to squeeze just the liver of the fish, but instead to squeeze the whole body of the fish, and collect the oil that comes out of the back passage. Needless to say, the alimentary tract is a very good source of the poisons of which the vertebrate body may wish to rid itself.
The third reason is that fish oil is rich in vitamin A. If taken in excess, vitamin A is toxic, and can even be fatal. Unfortunately, in order to obtain the levels of EPA needed to treat CFS the amount of fish oil that has to be consumed could be dangerous.
The fourth reason is that, in addition to containing EPA, fish oil also contains DHA.
DHA in supplement form is highly susceptible to lipid peroxidation. The renal products of this reaction are highly reactive free radicals that can damage DNA molecules.
In my view the best preparation to use in CFS patients and in any patients who suffer from sleep problems, tiredness or fatigue is VegEPA; each capsule contains 280 mg ultra-pure EPA, 100 mg virgin Evening Primrose Oil, and zero DHA. For adult patients, I prescribe eight capsules daily (unless the patient happens to be on blood thinning anticoagulant medication such as warfarin or heparin). As an added bonus, in the long-term, taking VegEPA regularly reduces the chances of your patient suffering from a heart attack, thrombotic stroke or deep-vein thrombosis. It is also very good for arthritis.
It is also important to encourage your patients to eat a varied and healthy diet that contains sufficient levels of certain vitamin and mineral cofactors that help with fatty acid metabolism. (These are also all contained within the vitamin and mineral supplement VegeCO, obtainable from the same sources as VegEPA; the adult dose is one VegeCO tablet daily, until the diet is adequate.)
One of the most delightful aspects of my job is seeing patients who have improved markedly on the above regime. Also, after just six to eight weeks of taking the fatty acid supplementation, do not be surprised if your patients find that their hair and nails are in better condition, and their skin looks and feels younger.
References
1. Puri BK. Chronic fatigue syndrome:A natural way to treat ME. Hammersmith Press. London. ISBN 1-905140-00-2. 2005.
2. Fukuda K et al. The chronic fatigue syndrome: a comprehensive approach to its definition and study. Ann Intern Med. 121: 953-959. 1994.
3. Behan PO et al. Effect of high doses of essential fatty acids on the postviral fatigue syndrome. Acta Neurol Scand. 82: 209-216. 1990.
4. Warren G et al. The role of essential fatty acids in chronic fatigue syndrome. Acta Neurol Scand. 99: 112-116. 1999.
5. Puri BK et al. Relative increase in choline in the occipital cortex in chronic fatigue syndrome. Acta Psychiatr Scand. 106: 224-226. 2002.
6. Chaudhuri A et al. Proton magnetic resonance spectroscopy of basal ganglia in chronic fatigue syndrome. Neuroreport. 14: 225-228. 2003.
7. Kaushik N et al. Gene expression in peripheral blood mononuclear cells from patients with chronic fatigue syndrome. J Clin Pathol. 58: 826-832. 2005.
8. Puri BK. The use of eicosapentaenoic acid in the treatment of chronic fatigue syndrome. Prostaglandins Leukot Essent Fatty Acids. 70: 399-401. 2004.
9. Puri BK et al. Eicosapentaenoic acid-rich essential fatty acid supplementation in chronic fatigue syndrome associated with symptom remission and structural brain changes. Int J Clin Pract. 58: 297-299. 2004.
10. Puri BK. Monomodal rigid-body registration and applications to the investigation of the effects of eicosapentaenoic acid intervention in neuropsychiatric disorders. Prostaglandins Leukot Essent Fatty Acids. 71: 177-179. 2004.
11. Puri BK. The clinical advantages of cold-pressed non-raffinated evening primrose oil over refined preparations. Med Hypotheses. 62: 116-118. 2004.
Further Information
VegEPA is available from www.vegepa.com or Tel: 0845 1300424.
Comments:
-
Linda said..
Not a comment for posting: just want to let you know you have a typo on your site:
"The enal products of this reaction are highly reactive..."
(Thank you for posting all that great info on good fats!)
Best regards,
Linda