Positive Health Online
Your Country

![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Lotus Books]](/img/original/TopicbannerAvatar/953.adb373b0210368e0c9ce4d9a8a9f01aa.jpg "Lotus Books")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
Osteopathic Approach to the Treatment of Thoracic Outlet Syndrome
listed in osteopathy, originally published in issue 190 - January 2012
Introduction
The most common cause is compression of the brachial plexus/subclavian artery (neuro-vascular bundle) as it passes through the 2 heads of scalene anterior and medius, which have become shortened, fibrous or in spasm. Usually as a result of trauma, sports injury i.e. scrum collapse, whiplash, fall; also first or second rib injury, nerve root irritation and chronic postural changes resulting in shortening of the scalene i.e. office workers, students, overtraining in sport (swimming/athletics), long-term smokers with hypertonic accessory muscles of respiration and patients with chronic kypho-lordosis of the cervico-thoracic region.

Seated Cervical Spine (CSP) High Velocity Thrust (HVT)
Also bony abnormality namely a cervical rib. This can be enlarged transverse process exostoses, hardened fibrous tissue and even a rudimentary rib protruding from the articular pillar of C7 (occasionally C6).
Clavicular fracture and resultant adhesion formation.
Signs and Symptoms;
Observation
- Head held forward;
- Visible hypertonic scalenes;
- Elevated first rib;
- Kypho-lordotic cervico-thoracic region;
- Evidence of clavicular fracture.
Sensory
- Parasthesia, numbness, tingling sensation in the arm & hand;
- Pain can be quite well defined following a specific dermatome i.e. C8 T1
- Medial aspect forearm, hand 5th digit & med half 4th digit.
Motor
- Decreased grip and hand strength. Weakness and wasting of the thenar hypothenar and interosseous muscles. In the acute phase the reflexes tend to be unaffected, but chronically they become reduced.
Vascular
- ↓ Radial Pulse, oedema, coldness, cyanosis, dry/excessive sweating;
- Raynauds sign, trophic changes, glossy skin, dry/damaged nails.
Differential Diagnosis
- Cervical spondylosis resulting in intervertebral foraminal encroachment of the nerve root(s);
- Cervical disc prolapse;
- Cervical facet capsular irritation;
- Trauma, fracture/severe ligament avulsion;
- Hypertonic pectoralis minor/coracobrachialis;
- Carpal/Guyon's tunnel syndrome;
- Osteo/rheumatoid arthritis.
Evaluation and Diagnosis
- Direct palpation to the articular pillar should reveal the presence of a cervical rib;
- Hypertonic cervical musculature may make palpation difficult ref(r)X-Ray/MRI;
- Adson's Test;
- Eden's Test;
- Roo's Test (abduction and external rotation test).
Top Tip; Be aware a ( pulse is quite common in asymptomatic patients, therefore do not just rely on one test several should be carried out to confirm.
Treatment
- ↓ Scalene hypertonia through soft tissue, Muscle Energy Technique (MET). This technique is best performed in a side lying position with the painful side uppermost. Ensure that the head and neck is well supported with the appropriate pillow. With the patient facing away from the operator, place one hand around the ear and occiput, whilst the opposite hand / arm is placed around the upper shoulder. The patient is then asked to lift their head up off the pillow against the resistance of the operator who simultaneously can pull down against the shoulder producing an isolytic stretch to the scalene muscles. Care must be taken not to push down hard against the patient's head, as this will cause excess side bending to the 'opposite' cervical facets potentially irritating them, especially if spondylosis is present.
- ↓ Cervical muscular hypertonia through soft tissue, MET, Inhibition, Counter strain techniques;
- Correct cervical, thoracic, and rib dysfunction through High Velocity Thrust (HVT), MET and articulation/traction techniques;
- Ice and NSAIDs during acute phase;
- Ultrasound pulsed at 0.5 W/cm² for 5-8 minutes over associated muscle tissue;
- Patient self-directed exercise programme to stretch associated muscle tissue. Namely scalenes, levator scapulae, trapezius. In patients with an anterior head and neck, exercise to tuck in chin and draw head posteriorly preferably standing against a wall will help to correct posture and stretch the anterior neck muscles.
Ward RC et al. Foundations for osteopathic medicine. 2nd edition.
Lippincott Williams and Wilkins, Baltimore. USA. 2002.
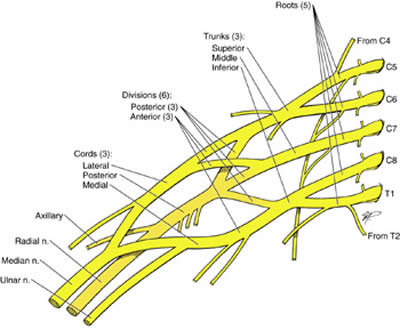
Injuries to the Brachial Plexus
Klumpke's Paralysis or Klumpke's Palsy or Dejerine-Klumpke Palsy
A form of brachial plexus injury in which there is paralysis of the muscles of the forearm and hand due to a childbirth injury to the roots of eighth cervical C8 and first thoracic T1 nerves or the lower part of the brachial plexus, a network of spinal nerves that originates in the back of the neck, extends through the axilla (armpit), and gives rise to nerves to the upper limb.
The risk is greater when the mother is small or when the infant is of large weight. The most common aetiological mechanism is caused by a traumatic vaginal delivery, necessitated by shoulder dystocia.
Symptoms
Symptoms include paralysis of intrinsic hand muscles, and ulnar nerve distribution numbness. Involvement of T1 may result in Horner's syndrome.
Erb's Palsy (Erb-Duchenne Palsy, Brachial plexus paralysis) is a paralysis of the arm caused by injury to the upper group of the arm's main nerves (specifically, spinal roots C5-C7), almost always occurring during birth. Depending on the nature of the damage, the paralysis can either resolve on its own over a period of months, necessitate physical therapy or require surgery.
The most common cause of Erb's palsy is dystocia, an abnormal or difficult childbirth or labour. For example, it can occur if the infant's head and neck are pulled toward the side at the same time as the shoulders pass through the birth canal. The condition can also be caused by excessive pulling on the shoulders during a vertex delivery (head first).
A similar injury may be observed in adults or following a traumatic fall on the side of the neck. It can also affect neonates affected by a clavicle fracture unrelated to dystocia. The paralysis can be partial or complete; the damage to each nerve can range from bruising to tearing. The most commonly involved root is C5 (aka Erb's point: the union of C5 & C6 roots), as this is mechanically, the furthest point from the force of traction, therefore, the first/most affected.
Symptoms
The most commonly involved nerves are the suprascapular nerve, musculocutaneous nerve, and the axillary nerve. The injury often leaves patients with stunted growth in the affected arm with everything from the shoulder though to the fingertips smaller than the unaffected arm. This also leaves the patients with impaired muscular, nervous and circulatory development. The lack of muscular development leads to the arm being much weaker than the unaffected one, and less articulate, with many patients unable to lift the arm above shoulder height unaided, as well as leaving many with an elbow contracture.
The lack of development to the circulatory system can leave the arm with an inability to regulate its temperature, which often proves problematic during winter months when it would need to be closely monitored, to ensure that the temperature of the arm was not dropping too far below that of the rest of the body. However the damage to the circulatory system also leaves the arm with another problem. It reduces the healing ability of the skin, so that skin damage takes far longer than usual to heal, and infections in the arm can be quite common if cuts are not sterilized as soon as possible. This will often cause many problems for children since they often injure themselves in the course of their childhoods.
The nervous damage is often the most problematic of the side effects to Erb's Pasly, but it is also the most varying. There have been cases of patients who have lost complete sensory perception within the arm after procedures whereas they had full sensory perception before. The most common area for a loss of sensory perception (except where the arm faces a total loss) is that between the shoulder and the elbow since the nerves which provide information from that area to the brain are also those first damaged in the initial causative trauma.
Bibliography
Chaitow L and Delaney JW. Clinical application of neuromuscular techniques. Volume 1: The Upper body. Churchill Livingston, England. 2002.
Greenman PE. Principles of Manual Medicine. 2nd Edition. Lippincott Williams and Wilkins. Baltimore. USA. 1996.
Kreider RB. Fry AC and O'Toole ML. Overtraining in Sport. Human Kinetics, Leeds, UK. 1998.
Magee D J. Orthopaedic physical assessment. 2nd edition. WB Saunders, Philadelphia, USA. 1992.
Pecina MM and Bojanic I. Overuse injuries of the musculoskeletal system. 2nd edition. CRC Press, London UK. 2004.
Subotnick S I. Sports medicine of the upper extremity. 2nd edition. Churchill Livingston, England. 1999.
Comments:
-
No Article Comments available