Positive Health Online
Your Country

![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: https://www.water-for-health.co.uk/]](/img/original/BannerAvatar/4046.12831f50177f8848ee87b8e94411d6b3.jpg "https://www.water-for-health.co.uk/")
![[Image: http://www.balens.co.uk]](/img/original/BannerAvatar/2148.50367fa908013fae0a7f1a171543ef92.jpg "http://www.balens.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
![[Image: Lotus Books]](/img/original/TopicbannerAvatar/953.adb373b0210368e0c9ce4d9a8a9f01aa.jpg "Lotus Books")
![[Image: Balens Specialist Insurance Brokers for Health & Wellbeing Professionals & Organizations]](/img/original/TopicbannerAvatar/3122.5661db4ab5e5bfd5fce3465edaa5662c.jpg "Balens Specialist Insurance Brokers for Health & Wellbeing Professionals & Organizations")
![[Image: ICAN International Clinical Aromatherapy Network]](/img/original/TopicbannerAvatar/4442.566a83a07de79de73b9c738f7fb6458a.jpg "ICAN International Clinical Aromatherapy Network")
The number of members of the medical and dental profession with NLP training has noticeably increased over the last few years. When I asked them how it has affected their lives, the response is "I don't know how I managed without it".
Neuro-Linguistic Programming – matured from the study of the internal processes of those people who excel in their chosen sphere of expertise or who have overcome a difficulty or illness.
Firstly the best psychotherapists were modelled and common patterns emerged which could be taught to others. Subsequently the modelling process was applied to the best salesmen, teachers, sportsmen, actors and many more.
One of the basic skills of NLP is the ability to recognise how people are thinking. For example: when a person is visualising he looks upwards to make pictures and uses language which tells you precisely how he is thinking, i.e. 'that looks good' or 'l see what you mean'. So when the best spellers were modelled it was immediately obvious that they were visualising the words and you know when you have taught a person to spell visually because seeing the word they can spell it as quickly backwards as they can forwards.
When people spell phonetically they often get it wrong because there are so many rules and exceptions to remember.
Most people in a kinaesthetic mode look down and right and say 'that feels good'. Any other eye movement represents internal language and expressions like 'that rings a bell' or 'sounds good to me'.
Modelling those people with a driving ambition to become something special, like a doctor or veterinary surgeon requiring a lot of self sacrifice and energy, it was found they had a vision or well formed outcome which enabled them to imagine what it would be like when they had attained what they wanted. Similarly the best patients, those who recovered from serious illness had a well formed outcome and a congruent belief in their ability to attain that outcome. Common patterns emerged which can be used to assist other patients on the road to recovery.
When Richard Bandler developed the Fast Phobia Cure he did not go out and study a bunch of phobics, he sought out people who had overcome a phobia and asked "How did you do that?" – It's unbelievably fast.
The Counter Example Allergy Process (see Positive Health issue 12), arguably the flagship of NLP as it is immediately demonstrable, was developed by Robert Dilts when an eminent Immunologist attending one of his health seminars made the remark that an allergy was like a phobia of the immune system, an overwhelming response to a harmless stimulus. If you were allergic to milk the counter example would be soya milk. We know that there is a lot going on at a neurological level because the allergic response can be brought on by a lifelike imitation of the allergen and multiple personalities have different allergies in different personalities. Worldwide NLP therapists get an 80% success rate and clinical trials are being carried out at Vail Medical Centre, Colorado.
There are no theories to NLP, only presupposition about what works:
(1) The map is not the territory
(2) Any behaviour however bizarre has a positive intention
(3) People have all the resources they need to get the outcome they want.
The map is not the territory
The world we live in is so rich in content that we cannot take in all the information presented to us. We have built in filters which select that information which we think is important, so we live in a world of our own selection. This world might be rich, friendly and empowering or frugal, hostile and limiting.
The information from the outside world is represented internally in a coded form to give it meaning.
My niece is a friendly, bubbly girl, very caring for others and with never an unkind word. She may get a bit peeved but not very angry. When I asked her "How do you do that?" she looked puzzled. So I said "Think of a happy event. What is it like?" As she thought of a happy event there was a change in her physiology as she smiled. I asked her to describe the internal pictures she was getting. "I have got big, bright pictures all around me." "Any noise?" "Yes, lots of happy voices and laughter." When I asked her to turn up the brightness and sound she began to enjoy it even more.
When I asked her to describe the internal pictures she got when recalling an uncomfortable event she described them as fuzzy, small and in the distance. These differences in perceptions or coding are called sub-modalities. The most important sub-modalities of the visual modality are locations, size, brightness – associated or disassociated. Associated is when you are in the event seeing it through your own eyes and disassociated is when you are seeing yourself in the event from the observer position. Associated is the more impactful creating a greater emotional response.
The NLP trauma/phobia cure involves creating a disassociated picture of the problem.
My niece is fortunate in that her brain presents her with large, emotive pictures of all the good things in life and small insignificant pictures of her problems. But what if her brain did the opposite and she had terrifying pictures of her problems, she would be a very different personality. There are NLP strategies to change submodalities. One way to help a person with depression would be to say "How precisely do you do that?" Their answer would tell you how to intervene.
Dental Phobia Cure
Fearful dental patients make internal pictures which depict dentists and their equipment as terrifying, which causes an overwhelming state of fear. The state can be reduced to an acceptable level by changing the submodalities. This can be done in a remarkably short space of time by a technique called 'the swish'.
The three steps of the swish are:-
(1) Create the cue picture.
(2) Create a desired self image which is attractive and motivating.
(3) Change submodalities of the cue picture to lessen its emotional impact.
Create the cue picture
1. To create the cue picture the patient is asked to imagine what she sees when she becomes frightened of a dental visit. The submodalities are intensified until she begins to feel the fear.
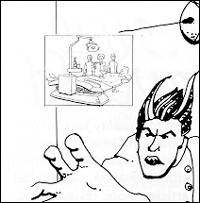
2. The desired self image is what the patient imagines she would look like after she has overcome her fear of the dentist. I would say "Imagine what you would look like when you have overcome your fear of the dentist, how would you be? That is you sitting over there, check her facial expression, notice the rhythm of her breathing."
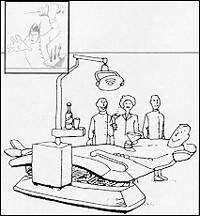
3. The swish is now used to change the submodalities of the cue picture. The patient is asked to interchange the cue picture and the desired self image in a special way until the cue picture has changed to something which is no longer frightening.
The figure above was drawn by a patient who had overcome her fear of the dentist. The big terrifying picture of the dentist has now changed (right) to a small fuzzy representation whilst she still has the self image of how she would like to be. This gives her brain something to move towards. The fear is now immediately replaced by the sense of comfort associated with the outcome picture. The process is remarkably fast, in fact, it doesn't work if you do it slowly.
The swish is one of the most useful tools in NLP. It can be used to overcome fears of flying, motorways, chemotherapy, hospitalisation and to change unwanted behaviours like smoking, overeating, getting in a rage or being jealous.
I would regard fear of flying as when the patient is able to board the aircraft maybe after a visit to the departure lounge bar. But a real flying phobic would be unable to board the aircraft. I have seen patients giving a history of having a panic attack on route to the airport and turning back or suddenly deciding not to go ahead when in the departure lounge.
The phobia cure is extremely fast and entails having the patient watch herself as she watches herself go through the phobia experience. A simple strategy to do this involves having the patient imagine she is in the projection booth (controlling the projector) as she watches herself in the stalls watching herself on the screen. She now changes the submodalities of the phobic experience on the screen by manipulating the projector until she feels comfortable with the picture on the screen.
Consider the scenario of two people who have decided to fly to the sun for a holiday. They have never flown before and both have a preferred representational system which is visual. They have looked at all the brochures, listened to friends and both have formed a vision or internal picture of what they want – and it feels good.
Before the holiday there is an air crash depicted on television and all the newspapers, which they both see.
Person A has a brain which presents an internal picture of the event which is small, fuzzy and in the periphery of his internal vision.
Person B's brain presents an internal picture of the crash which is big, bright and panoramic.
There are no prizes for guessing who will be visiting his doctor for a prescription or spending time in the departure lounge bar.
Or person B might go to an NLP therapist. A therapist who knows how to use language to help therapy would say What was the problem you have been having?
Well, I have booked this holiday and since I saw this air crash on television I can't go ahead with it.
How does this air crash stop you going on holiday?
I'm terrified.
Can we try to see what happens?
The therapist now knows precisely what this patient wants and can use 'the swish' which will reduce the power of the limiting picture and intensify the outcome – Person B on holiday – it takes minutes.
Our internal perceptions of time need submodalities so that we can differentiate between events that have really happened and events we imagine may take place in the future.
To illicit a time-line I would say "think of an event which is a daily routine – like tooth brushing and think about tooth brushing today and point to the picture you get". Then I would have them repeat the process for a week ago, a year ago and five years ago and then at the same intervals of time into the future. They may say "well it's in my head". Well it is but it will occupy a space in your psychogeographical world. By plotting the location on paper you will now have a map of how they represent time. Most right handed Europeans represent the past to the left and the future to the right. How we represent time will have a dramatic effect on our external behaviour. Some people represent the past as a short compressed time line in front of them, they tend to live in the past, have difficulty with decisions because problems keep representing themselves, have past traumatic events continually in focus and in my experience suffer post traumatic stress and persistent pain syndrome.
On the other hand those people with the past behind them appear to sail through life, decision making is easy, overcoming relationship problems and setbacks as they put the events behind them. Some people have time-lines which are conducive to future planning and you may think, I like the way he plans his life and you could ask him "How do you do that?" You could then model his time-line and try it out for yourself on a temporary basis (preferably in the safe haven of a training seminar). Those people with past and future behind them are often delightful company as they live entirely in the present but as they don't tend to learn from the past and the future holds no consequences, they may behave irresponsibly.
Dyslectics have a very confused time-line and can be helped by changing it so that the past is well separated from the future.
Any behaviour, however bizarre, has a positive intention
Or we get some benefit from it. This is why it is so difficult to change behaviours and to do so it is necessary to consider the benefits the patient derives from the behaviour. People get all sorts of benefits from smoking such as comfort, relaxation, diversion from an ongoing problem or a feeling of being grown up. Once it is accepted that having a symptom as a behaviour it is possible to help many patients with such problems as asthma, migraine, eczema and many more.
Examples in my experience were: an asthma attack attracted recognition, a migraine avoided a boring shopping trip, eczema solved an ongoing personal problem and M.E. gave a man an excuse to stay at home and attend to the needs of an ailing wife. It is as if a part is prepared to go to any lengths to get what it wants.
The strategy for change is to assist the patient to come up with a new behaviour that will get the same benefit, it is called reframing. A lady rang me and queried how I could possibly cure migraines at one visit. I explained about behaviour and positive intentions, as she put the phone down she did not sound very convinced. She rang me a week later to thank me for curing her migraine. Apparently the prospect of showing someone around the house which she had put up for sale brought on a migraine. There was a part of her which wanted to keep the house and was prepared to go to any extreme to get what it wanted.
People have all the resources they need to create the outcome they want
Before any NLP changework, it is necessary to have the patient describe in sensory terms what he wants – what he will see, hear and feel when he has what he wants, it is not dependent on anybody else. The task of an NLP therapist is to guide the patient to a well formed outcome and to access the resources he needs.
Problem —> Resources —> Desired State
The resource is often at the heart of the problem.
This is best illustrated by an example.
The patient (a schoolmaster) presented with the problem, part of him wanted to be a woman. This was not how he identified himself and was a source of a lot of internal conflict. The therapy went like this:
How do you know you want to be a woman – what does it feel like?
I get a pressure in my stomach – like something trying to get out.
Imagine what that pressure would look like if you could see it.
Surprise – It's me dressed as a woman!
If it had a voice what would it sound like?
Sounds like an Aunt – she is dead now.
Now this part of you is a much younger you and a part you have tried to ignore and push away from you. Be kind to it, make it feel welcome and ask it what it is it wants from you.
It wants me to be a loving person.
Thank it for communicating with you and ask it if having you be a loving person, what would it want for you that is even more important than that.
It wants me to be in a loving relationship.
Again thank it and ask having got that what would it want for you.
Peace of mind.
Peace of mind is the resource and is a very powerful core state on a spiritual level and the patient has taken on a very relaxed physiology, his breathing is regular, he is very relaxed and probably feels very powerful. Other core states might be OKness, grounded or peace with God and descriptions vary from 'my road to Damascus', 'floating high on a cloud', or like 'watching a sunrise from a mountain top'.
And having peace of mind as a way of being in the world how does that change and transform wanting to be a woman so that you can have a loving relationship?
There followed a very emotional moment of enlightenment as the patient realised he no longer needed to be a woman so that he could have a loving relationship.
The part of him that wanted to be a woman was formed when as a young boy he overheard the remark 'only women can truly love another person'. A younger part of him wanted a loving relationship for him and was prepared to go to any length to get it!
Other unwanted behaviours have their origins at an identity level. Our immune system is part of our identity recognising self and non-self. Any identity crisis such as occurs after a bereavement or rapid change will affect the immune system functioning resulting in auto-immune diseases or persistence of abnormal malignant cells. Accessing a core state will give the immune system its best chance and aid conventional treatment on the road to recovery.
World wide there are repeated cases of improvements of patients with auto-immune diseases benefiting from NLP intervention but as these treatments are rarely carried out in isolation they must remain anecdotal.
Comments:
-
No Article Comments available