Positive Health Online
Your Country

![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Organic Aromatherapy]](/img/original/TopicbannerAvatar/1001.12a011c5d14492e86a5a2fa985244b74.jpg "Organic Aromatherapy")
![[Image: Human Kinetics Trail Guide to the Body]](/img/original/TopicbannerAvatar/4656.d9ccc329faa3d1500b4807b369feccef.jpg "Human Kinetics Trail Guide to the Body")
![[Image: Lotus Books]](/img/original/TopicbannerAvatar/953.adb373b0210368e0c9ce4d9a8a9f01aa.jpg "Lotus Books")
![[Image: ICAN International Clinical Aromatherapy Network]](/img/original/TopicbannerAvatar/4442.566a83a07de79de73b9c738f7fb6458a.jpg "ICAN International Clinical Aromatherapy Network")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
![[Image: SG Cancer Book]](/img/original/TopicbannerAvatar/960.4f24bbd158abe4427cc06911969143e5.jpg "SG Cancer Book")
Letters to the Editor Issue 220
listed in letters to the editor, originally published in issue 220 - February 2015
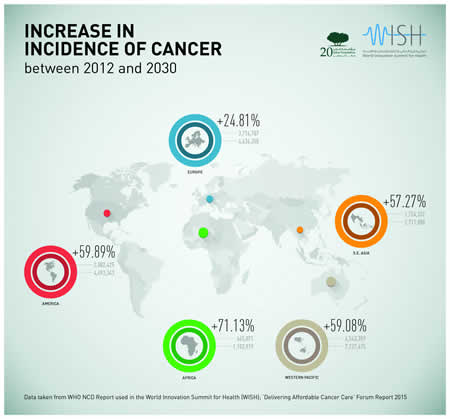
Report Highlights Rising Global Cost Of Cancer Treatment And Care
Authors of new report being presented in February call on governments and healthcare professionals to address rising cost burden of cancer care
Worldwide spending on cancer has now reached levels equivalent to the GDP of Hong Kong, the 35th largest economy in the world. This is just one of the shocking statistics highlighted in a new report being presented at the World Innovation Summit for Health (WISH) in Qatar later this month (17-18 February).
To mark World Cancer Day (4 February), the authors of the report are releasing early findings to help drive awareness of the global cancer burden, shining a light on the true scale of the problem and calling on governments, policymakers and healthcare organisations to tackle the rising cost of the disease. World Cancer Day is a day dedicated to raising global awareness about the disease in order to harness and mobilise solutions and bring about positive action at an individual, community and governmental level.
The WISH report will highlight that health economies worldwide are expecting increases of 16–32 per cent in new cancer diagnoses over the next 10 years and projections from the US, United Kingdom and Australia suggest that cancer costs in these countries could increase by as much as 42–66 per cent above current levels by 2025.
With the continual development of new treatments and high-profile debates raging about how patients are selected for expensive drugs, the report will also present evidence that in many cases, cancer could be treated very differently and that there are too many instances of over-treatment and needless use of expensive technology. The report will highlight innovative projects from around the world that have driven efficiencies and improved treatments for patients.
Professor Robert J S Thomas, ‘Delivering Affordable Cancer Care’ WISH Forum Chair, said:
“Our aim is to develop a plan to encourage governments, policymakers and large healthcare organisations to take up and recognise the problem of affordability. It is a really key issue for patients at all levels and a key issue for governments. Everyone is worried about the high cost of cancer care. What we want is a plan which will help patients in the long term.”
Commenting on the significance of World Cancer Day, Professor the Lord Darzi of Denham, Executive Chair of WISH and Director of the Institute of Global Health Innovation at Imperial College of London, said: “The challenge of cancer is daunting and it will intensify. World Cancer Day provides a platform for people worldwide to reflect on the impact that the disease has on millions of lives globally. As populations age, more people are developing cancer, they are surviving longer with it and treatment costs are soaring. The only way to help patients get the treatment they need is to ensure that money is spent effectively. This report brings together the greatest minds in the field of cancer care to help policymakers and healthcare professionals find solutions to address the significant cost and health consequences of this unforgiving disease.”
Through its support of World Cancer Day, WISH, an initiative of Qatar Foundation for Education, Science and Community Development, highlights QF’s mission to inspire and promote healthcare development and reform through a global network of high-level policymakers, academics and industry leaders. WISH remains closely aligned to the vision and mission of QF to unlock human potential and underscore Qatar’s pioneering role as an emerging centre for healthcare innovation.
Other Key Findings from the WISH Report:
- Cancer is responsible for 5–7 per cent of healthcare costs in high-income countries and reached approximately USD290 billion per year in 2010;
- Cancer is the second largest contributor to the non-communicable disease burden;
- It is estimated that, from 2008 to 2030, cancer incidence will rise by 65 per cent in high-income countries, 80 per cent in middle-income countries, and 100 per cent in the world’s poorest countries;
- There were 13.3 million new cases of cancer in 2010, with the number projected to rise to 21.5 million in 2030.
Watch Prof. Robert Thomas introduce his WISH 2015 report on Affordable Cancer Care https://www.youtube.com/watch?v=y3rZSWZA8b4
Further Information
For more information about WISH or the 2015 Summit, please visit www.wish.org.qa
The Disney Measles Outbreak: A Mousetrap of Ignorance
by Sayer Ji, Founder GreenMed Info
While the Disney measles outbreak is being blamed on the non-vaccinated, the evidence reveals a failing measles vaccine is behind the outbreak. The latest stratagem to blame a failing measles vaccine on the non-vaccinated is all over the mainstream media, or should we say the marketing and cheerleading arm of the vaccine industry and the medical-industrial complex.
Two years ago, while a similar debacle was being played out, I wrote an article titled, The 2013 Measles Outbreak: A Failing Vaccine, Not A Failure To Vaccinate, which deconstructed the myth that the minimally- or non-vaccinated were responsible for outbreaks of measles in highly vaccination compliant populations. According to the prevailing propaganda it is fringe religious communities, visitors from countries where measles is common, and vaccine objectors within the United States, that are responsible for the failure of the measles vaccine to confer lasting immunity.
Looking at the rising tide of vaccine resistant infectious outbreaks in the U.S. and abroad --chickenpox, shingles, mumps, whooping cough (pertussis), influenza, HPV (Gardasil), hepatitis B, to name but a few - through the lens of the peer-reviewed and published literature on the topic, it is clear that the vaccines and not those who refuse to subject themselves to them are at the root of the problem. And nowhere is this more clearly evident than in the measles vaccine.
How do we Know This?
Just a few months ago, a study published in PLoS titled Difficulties in eliminating measles and controlling rubella and mumps: a cross-sectional study of a first measles and rubella vaccination and a second measles, mumps, and rubella vaccination brought to light the glaring ineffectiveness of two measles vaccines (measles-rubella (MR) or measles–mumps–rubella (MMR) ) in fulfilling their widely claimed promise of preventing outbreaks in highly vaccine compliant populations. We dove deeply into the implications of this study in our article titled Why Is China Having Measles Outbreaks When 99% Are Vaccinated?
Also, as we have explored in a previous article, Measles: A Rash of Misinformation, the measles vaccine is not nearly as safe and effective as is widely believed. Measles outbreaks have consistently occurred in highly immunization compliant populations. Here are just a few examples reported in the medical literature:
- 1985, Texas, USA: According to an article published in the New England Journal of Medicine in 1987, "An outbreak of measles occurred among adolescents in Corpus Christi, Texas, in the spring of 1985, even though vaccination requirements for school attendance had been thoroughly enforced." They concluded: "We conclude that outbreaks of measles can occur in secondary schools, even when more than 99 percent of the students have been vaccinated and more than 95 percent are immune."[1]
- 1985, Montana, USA: According to an article published in the American Journal of Epidemiology titled, "A persistent outbreak of measles despite appropriate prevention and control measures," an outbreak of 137 cases of measles occurred in Montana. School records indicated that 98.7% of students were appropriately vaccinated, leading the researchers to conclude: "This outbreak suggests that measles transmission may persist in some settings despite appropriate implementation of the current measles elimination strategy."[2]
- 1988, Colorado, USA: According to an article published in the American Journal of Public Health in 1991, "early 1988 an outbreak of 84 measles cases occurred at a college in Colorado in which over 98 percent of students had documentation of adequate measles immunity ... due to an immunization requirement in effect since 1986. They concluded: "...measles outbreaks can occur among highly vaccinated college populations."[3]
- 1989, Quebec, Canada: According to an article published in the Canadian Journal of Public Health in 1991, a 1989 measles outbreak was "largely attributed to an incomplete vaccination coverage," but following an extensive review the researchers concluded "Incomplete vaccination coverage is not a valid explanation for the Quebec City measles outbreak.[4]
- 1991-1992, Rio de Janeiro, Brazil: According to an article published in the journal Revista da Sociedade Brasileira de Medicina Tropical, in a measles outbreak from March 1991 to April 1992 in Rio de Janeiro, 76.4% of those suspected to be infected had received measles vaccine before their first birthday.[5]
- 1992, Cape Town, South Africa: According to an article published in the South African Medical Journal in 1994, "[In] August 1992 an outbreak occurred, with cases reported at many schools in children presumably immunised." Immunization coverage for measles was found to be 91%, and vaccine efficacy found to be only 79%, leading them to conclude that primary and secondary vaccine failure was a possible explanation for the outbreak.[6]
These six outbreaks are by no means exhaustive of the biomedical literature, but illustrate just how misled the general public is about the effectiveness of measles vaccines, and the CDC's vaccination agenda in general. No amount of historical ignorance will erase the fact that vaccination does not equal immunization; antigenicity does not equal immunogenicity.
The superstitious and ironically non-evidence-based faith in the infallibility of vaccines speaks volumes as to why the growing movement to educate the public about the true nature of vaccines is increasingly labelled "anti-vaccine," when in fact it is pro-vaccine awareness, namely, making the public aware of vaccine failures and the growing plight of the countless vaccine injured around the world.
UNICEF and the Bill & Melinda Gates Foundation can continue to label those who bring the peer-reviewed 'evidence' to the public's attention as 'liars' or 'child killers, as Bill Gates did in a CNN interview with Dr Sanjay Gupta. But all this does is to increase the public's suspicion of the real agenda behind their ostensibly charitable plea to save the poor and the needy from the hell of disease, instead of focusing on improving their most basic living conditions, nutrition, sanitation, refrigeration, etc., and making inroads to reduce the geopolitical violence that is ruining the lives of hundreds of millions.
Measles is a real disease with real adverse health effects, some of which can be life threatening in the already immunocompromised (vaccination representing a major cause of TH1/TH2 imbalances). But it is our immune status, as with all infectious diseases, that determines susceptibility and whether or not a disease will be mild or lethal. You can't vaccinate away conditions that lead to compromised immunity, nor can you 'immunize' folks -- especially parents - against the desire to pursue the truth about vaccines. Learn more on our research vaccine database: Health Guide: Vaccine Research.
References
1. T L Gustafson, A W Lievens, P A Brunell, R G Moellenberg, C M Buttery, L M Sehulster. Measles outbreak in a fully immunized secondary-school population. N Engl J Med: 316(13): 771-4. PMID: 3821823 Mar 26 1987.
2. R M Davis, E D Whitman, W A Orenstein, S R Preblud, L E Markowitz, A R Hinman. A persistent outbreak of measles despite appropriate prevention and control measures. Am J Epidemiol 126(3):438-49. PMID: 3618578. Sept 1987.
3. B S Hersh, L E Markowitz, R E Hoffman, D R Hoff, M J Doran, J C Fleishman, S R Preblud, W A Orenstein. A measles outbreak at a college with a prematriculation immunization requirement. Am J Public Health. 81(3):360-4. PMID: 1994745 Mar 1991.
4. N Boulianne, G De Serres, B Duval, J R Joly, F Meyer, P Déry, M Alary, D Le Hénaff, N Thériault.[Major measles epidemic in the region of Quebec despite a 99% vaccine coverage]. Can J Public Health. 82(3):189-90. PMID: 1884314. May-Jun 1991.
5. S A de Oliveira, W N Soares, M O Dalston, M T de Almeida, A J Costa. Clinical and epidemiological findings during a measles outbreak occurring in a population with a high vaccination coverage. Rev Soc Bras Med Trop. 28(4):339-43. PMID: 8668833 Oct-Dec 1995.
6. N Coetzee, G D Hussey, G Visser, P Barron, A Keen. The 1992 measles epidemic in Cape Town--a changing epidemiological pattern. S Afr Med J. 84(3):145-9. PMID: 7740350 Mar 1994.
Source and Further Information
Reproduced from Sayer Ji. www.GreenMedInfo.com
www.greenmedinfo.com/blog/disney-measles-outbreak-mousetrap-ignorance?page=1
www.greenmedinfo.com/blog/disney-measles-outbreak-mousetrap-ignorance?page=2
British Court Throws Out Conviction of Autism/Vaccine MD: Andrew Wakefield’s Co-Author Completely Exonerated
Posted By Site Admin March 2012
Facebook Posting by Martin Walker
Better late than never as they say. But I do wish that people would contact me about the many essays I wrote during the GMC hearing - of which I attended every day. My essay Lots of Law but Little Justice about the appeal hearing of Walker-Smith written in 2012 can be obtained for free from me. www.slingshotpublications.com/essays/lots-of-law-but-little-justice
www.facebook.com/frakatime?fref=nf
In a stunning reversal, world renowned pediatric gastroenterologist Prof. John Walker-Smith won his appeal against the United Kingdom’s General Medical Council regulatory board that had ruled against both him and Andrew Wakefield for their roles in the 1998 Lancet MMR paper, which raised questions about a link to autism. The complete victory means that Walker-Smith has been returned to the status of a fully licensed physician in the UK, although he had already retired in 2001 - six years before the GMC trial even began.
Justice John Mitting ruled on the appeal by Walker-Smith, saying that the GMC “panel’s determination cannot stand. I therefore quash it.” He said that its conclusions were based on “inadequate and superficial reasoning and, in a number of instances, a wrong conclusion.” The verdict restores Walker-Smith’s name to the medical register and his reputation to the medical community. This conclusion is not surprising, as the GMC trial had no actual complainants, no harm came to the children who were studied, and parents supported Walker-Smith and Wakefield through the trial, reporting that their children had medically benefited from the treatment they received at the Royal Free Hospital.
While John Walker-Smith received funding to appeal the GMC decision from his insurance carrier, his co-author Andrew Wakefield did not - and was therefore unable to mount an appeal in the high court. This year, however, Dr. Wakefield, who now conducts his research in the US, has filed a defamation lawsuit against Brian Deer, Fiona Godlee and the British Medical Journal for falsely accusing him of “fraud.” The suit is currently underway in Texas, where Wakefield now lives. The ruling today bodes well for Dr. Wakefield’s suit against Deer, on whose reporting the entire GMC hearing was based.
In 1998 the Lancet published a case series on twelve children receiving treatment for bowel dysfunction at the Royal Free Hospital in London. The paper called for further study of a possible association between bowel disease and developmental delay, including cases of autism. It also noted that eight of the children’s gastrointestinal and autistic symptoms began shortly after they received the MMR vaccination. The verdict today raises questions about whether or not the Lancet should have retracted the paper after the GMC decision, as the reasons for its retraction have now been contradicted by the judge’s decision.
The thirteen original co-authors of the 1998 Lancet case series were members of the Royal Free’s Inflammatory Bowel Disease Study Group. In 2004, under pressure from the British medical establishment, ten of the co-authors signed a letter retracting an interpretation of the paper that it proved that vaccines caused autism, which the paper never actually claimed in the first place. John Walker-Smith, Andrew Wakefield and Dr Simon Murch were subsequently brought up on misconduct charges before the GMC. The proceedings resulted in Walker-Smith and Wakefield being found guilty and being ‘struck off’ the medical register, while Dr Murch retained his status as a physician. Wakefield was then vilified by corporate media and by bloggers eager to repeat scandal and engage in industry protectionism, rather than investigate the complicated facts of the story.
Today, almost 14 years after the paper was published, the high court determined that John Walker-Smith was innocent of the wrongdoing alleged by the GMC. Judge Mitting reported that the GMC, “on the basis of sensible instructions, does not invite me to remit it to a fresh Fitness to Practice panel for redetermination. The end result is that the finding of serious professional misconduct and the sanction of erasure are both quashed.”
British parents from the group CryShame, which includes parents of the Lancet 12, issued a statement saying that they “welcome with immense relief the end of the eight year ordeal of Prof John Walker-Smith and the quashing of all substantive charges against him in the High Court, and wish him their heartfelt congratulations at finally clearing his name.”
“Though justice has finally prevailed for Prof. Walker-Smith, the damage done to him and his colleagues has been incalculable,” said Mark Blaxill, chairman of the Canary Party. “The UK government must investigate the corruption in the GMC, which has severely damaged the reputations of good, honest doctors. Most of all, it’s outrageous that Dr Andrew Wakefield has been vilified by government officials, vaccine manufacturers and physician organizations, and that the media has accepted these unfounded accusations uncritically.”
“It’s time that we started treating responsible parents as reliable witnesses to serious adverse reactions to medical procedures such as vaccination,” said Jennifer Larson, president of the Canary Party. “The work that Walker-Smith and his colleagues at the Royal Free Hospital did with the Lancet 12 was medically necessary and above reproach. No patient complained, and the charges against the Royal Free team came only from a freelance journalist writing for a Rupert Murdoch newspaper. Meanwhile, the findings reported in the Lancet paper have been replicated in numerous scientific publications and reported by thousands of parents all over the world.”
“It is quite obvious to me that James Murdoch, Brian Deer and GlaxoSmithKline orchestrated the smear attack on Dr Andrew Wakefield,” said Ginger Taylor, executive director of the Canary Party. “A judge has now ruled that the GMC hearings were a farce. Parents are waiting for journalists to find their spine and start some honest reporting on the character assassination of doctors that is blocking medical treatments for vaccine injured children, and the role that GSK and Merck may be playing to protect their profits on the MMR vaccine. The Canary Party honours and stands by doctors of integrity like Prof. Walker-Smith, who continue to fight and defend their hard-won reputations for going the extra mile to investigate and improve the chronic, difficult-to-treat cases that now permeate our society.”
Sources:
Martin Walker on Facebook: www.facebook.com/frakatime?fref=nf
It 'CAM' and Should Be a Part
by Rajgopal Nidamboor
It is time we integrated complementary, evidence-based medicine into the allopathic, or conventional, medical curriculum through research and nutrition, to bring about a gentle, humanistic approach to healthcare.
The idea of incorporating and teaching complementary and alternative medicine (CAM) in the conventional medical school curriculum has been a raging debate for too long. The argument is not so much as to whether or not conventional medical institutions are receptive enough to integrate evidence-based CAM knowledge in their own academic or clinical setting, or whether CAM should be a part at all. What is imperative is a balanced view, because the community at large expects medical professionals to be able to provide information and guidance about the quality and therapeutic use not just of conventional medicine, but also complementary, integrative or functional medicine, which most patients use some time or other.
CAM is a term used for different complementary and alternative medical practices and medicines. There is more than definitive therapeutic and scientific evidence for a number of them, albeit sceptics often ‘sweep them off the ground’ as being just placebo. The fact is that, any which way you look at it, a host of CAM modalities are derived from ancient sciences. Ayurveda, the Indian system of medicine, for instance, has a long history of successful traditional use.
Many sceptics likewise consider homeopathy, a growing CAM approach, as pseudoscientific ‘mumbo-jumbo’. They argue that it shouldn’t be taught at the university level, or in CAM protocols in conventional medical schools. There is adequate evidence for homeopathy as a clinically effective mode of treatment for several conditions, ranging from allergies and skin diseases to functional disorders, such as irritable bowel syndrome (IBS), to name a few. What’s more, studies have demonstrated that homeopathy, when used as an adjuvant with conventional medicine, is more effective than treatment outcomes with the latter alone. This relates to conditions such as diabetes, hypertension, and arthritis, apart from hormone replacement therapy (HRT), among others. The question is: why shouldn’t conventional medical students and practitioners learn about such evidence and apply the Ayurvedic, or homeopathic, option to augment treatment choices and improve patient outcomes?
Well, sceptics again may have their own purpose for stalling the idea; they may also ask for more evidence and expanded evidence. Yet, there could be a way out of the impasse - because it certainly won’t take long to establish review boards to identify what CAM information resources are of high-quality, evidence based, unbiased, well structured, or flawed. There are certain high-quality CAM resources already accessible; they are also a part of educational curricula and research at universities. They could be scaled up and meta-analyzed.
Many factors also highlight the rationale for greater attention to CAM in undergraduate medical education (UME). They are, in précis:
- The widespread use of CAM by patients and their projected increase over the next decade;
- A majority of CAM users continue to use conventional medicine, creating potential safety risks due to medicinal interaction effects;
- Only a minority of patients reportedly disclose CAM use to their conventional physicians;
- Patients report wanting to receive information about CAM from their physicians;
- The growing evidence base for certain CAM therapies.
The best place for medical and health professionals to accrue knowledge is at the university during their academic studies. The best advantage universities possess is the close relationship that exists between research and teaching. Besides, students are better engaged and inspired by research-led teaching, especially research provided for queries while teaching. It is therefore not surprising that a handful of universities in the West research CAM to generate evidence-base and/or disprove its efficacy.
So, why the dichotomy to block CAM in conventional schools, as some sceptics would want? The CAM riposte is obvious: why support research, when one excludes teaching of CAM in conventional medical schools or universities? All one needs is intent, or the will to translate CAM research results into better CAM practices for everyone’s benefit. The best mode is to start teaching new conventional medical practitioners the uses, or the downside, of CAM in a given situation or condition.
The point today, or in the future, is not so much whether conventional medical students who learn about CAM approaches ever incorporate CAM in their practice. The big point is that they certainly stand to gain from viewing medicine in a more holistic manner, not with dark glasses. As a Texas medical student said in a newspaper interview, “It’s ironic ... as medical students, we approach our education as scientists who make decisions on evidence and fact. But, learning about CAM has really led me back to the humanistic part of medicine...”
This is a shorter version of the article that was first published in ©Townsend Letter, December 2014.
To download and read the full article, click here
www.4shared.com/office/qzJPC8A5ce/Rajgopal_Nidamboor-CAM-Townse.html
www.4shared.com/web/preview/pdf/qzJPC8A5ce0
Further Information
Rajgopal Nidamboor may be contacted via editor@health-prism.com
Websites: www.health-prism.com / www.upanishabd.com
Personal blog: www.wordoscope.com
The Cancer Act of 1939 - Outdated
Many people are unaware that this outdated Cancer Act Chapter 13, section 4 exists. It states that it is illegal for anyone to advertise or practice any cancer treatment apart from surgery, chemotherapy and radiation. It is also illegal to make any claims about cures or potential cures using complementary / alternative or integrated health methods.[1]
There are a range of complementary therapies which greatly help the prevention of cancer cells from forming and which also can give relief to those already suffering from cancer: meditation, visualizations, Reiki and other relaxing hands on therapies, and not forgetting diet and lifestyle. All these therapies can be used alongside the allopathic [conventional] treatments OR as an alternative, but we are legally not allowed to make people aware of this and we certainly cannot make any claims.[2-4]
There is a lot of very important scientific research going on and this is very valuable, for example: Dr Dylan Edwards from the Norwich Research Park studies the inherited genetics of cancer.[5] An estimated £600 million is spent on cancer research every year[6-7] and this is mostly spent on searching for drugs that will kill the cancer cells, whereas we should surely be looking for ways of preventing cancer cells from forming in the first instance..
Why are we not researching and educating people in ways to PREVENT cancer?
Many individuals have benefitted from taking vitamin B17 or Laetrile, Essiac tea, mistletoe injections and even coffee enemas; in fact some people have actually destroyed the cancer cells completely using these alternative methods, sometimes in conjunction with various therapies.[3,8]
Recently the Chairman of the Parliamentary Group for Integrated Healthcare, MP David Tredinnick, who has been a long time supporter of complementary therapies, participated in the Ministry of Health Committee meeting.
But we still have this outdated Cancer Act. When is it going to be brought up to date?
Sincerely
Christine Johnston, Therapist
References
1. UK 1939 Cancer Act:
www.legislation.gov.uk/ukpga/Geo6/2-3/13/contents
www.legislation.gov.uk/ukpga/Geo6/2-3/13/section/4
http://en.wikipedia.org/wiki/Cancer_Act_1939
2. Krebs, Ernst T. & Ernst T. Krebs, Jr., "Hexuronic acid derivatives" Dr Krebs. Cancer News Journal. May/August, 1970 and The Nitrilosides in Plants and Animals, "Nutritional and therapeutic Implications", Krebs E.T, Cancer Book House, Los Angeles, California, USA. Published by the Cancer Control Society, a non-profit educational Society dedicated to educating the public about nutrition and non-toxic cancer therapies.
3. Carl O Helvie RN DrPH . You Can Beat Lung Cancer Using Alternative / Integrative Interventions. Ayni Books. 2012
4. Griffin G Edward. The Science and Politics of Cancer Treatment. American Media. 2011.
5. www.uea.ac.uk/biological-sciences/people/profile/dylan-edwards
7. www.publications.parliament.uk/pa/ld200910/ldselect/ldsctech/104/104we56.htm
8. Gillian Gill. Take Control and Live. 2014. Gillian Gill. www.amazon.co.uk/TAKE-CONTROL-LIVE-Gillian-Gill/dp/095631211X
Essiac Tea - CancerTruth
HEALTH TIP: Back in 1922, a Canadian nurse named Rene Caisse noticed some scar tissue on the breast of an elderly woman. The woman told her that doctors had diagnosed her with breast cancer years before. However, the woman didn’t want to risk surgery, nor did she have the money for it. Providentially, she had met an Ojibway Indian medicine man who told her that he could cure her cancer with an herbal tea. The woman proceeded to tell Caisse about the ingredients in the tea. About a year later, Caisse was walking beside a retired doctor who pointed to a common weed and stated, “Nurse Caisse, if people would use this weed there would be little or no cancer in the world.” This ‘weed’ (sheep sorrel) was one of the herbs in the medicine man’s formula. The doctor had watched his horse cure itself of cancer by repeatedly grazing in a particular part of the pasture where sheep sorrel grew.
In 1924, Caisse wanted to test the tea on her aunt who had been diagnosed with terminal stomach cancer and was given less than six months to live. Caisse asked the physician Dr RO Fisher, for permission to try the tea on her aunt, and he consented. Her aunt drank the herbal tea daily for two months and recovered. Amazingly, she lived for 20 more years! Caisse also tested the tea on her mother who had been diagnosed with terminal liver cancer and had been given less than two months to live. Remarkably, her mother lived another 18 years!
What was in the tea? Well, technically, Essiac Tea is not a tea, rather it is a decoction of herbs, since the herbs are boiled and then steeped for several hours. In order to be true Essiac it must always contain the four essential herbs: Burdock Root, Sheep Sorrel, Slippery Elm Bark, and Turkish Rhubarb Root. She named the tea “ESSIAC” (which is Caisse spelled backwards). Essiac Tea is now used all over the world by cancer patients who want to avoid chemo and radiation. My own grandmother lived for over a decade with ‘terminal’ cancer and her primary daily treatment was Essiac tea.
with Susan SeppiVan, Charlene White, Tina De Francesco and 46 others
Further Information
The Cancer Mavericks shared CancerTruth's photo
There's a brand known as 'Flor essence' which is very similar to Essiac tea and is stocked at many health food shops or online:
www.bodykind.com/…/60-Flor-Essence-Detox-Tea-500ml-L…
Conspicuous Fitness versus Unhealthy Dependency
by Edwin Alan Salter PhD
Our very polarized society makes its divisions obvious. The phrase 'conspicuous consumption' has already been used (by Veblen) to describe ostentatious excess, and 'survival of the fittest' is an accolade bestowed on itself by entrepreneurial capitalism. The emergence of this dominating class requires as its economic complement a far more numerous population that stagnates or sinks toward poverty; a new underclass, denigrated as stupid and bad, serves as the contrast that justifies the advantages of the ultra-rich.
Wealth proclaims all merits, including the health shown by apparent fitness. The very richest, a fraction of one percent, associate themselves with exclusive sports - yachting, polo, flying, horse racing - though they require no practical physicality or skills beyond their class membership. They display bodies well cared for and not fat, and wear expensive fabrics and styles demonstratively unsuited to the mundane world, its tasks and difficulties. Riches, especially from privilege and undeserved luck, easily corrupt, but we are so admiring of their wonderful achievement (the association with psychopathy is well established and some greedy accumulation may be a variety of OCD) that it doesn't notice. Their world is protected and most of us merely glimpse it through the surrounding commerce of speculative finance, thin fashion models and gated residences. They assert status powerfully and believe in the fictions of money and the values of their microcosm. They don't intend to change and will ensure their children are like themselves. If they want to feel even better they can buy any amount of treatment and endorsement.
The poorest deteriorate: insecure, harried by debt and consuming foolishly for some sense of comfort, they slip into the most unhealthy ways of living, leading toward inactive obesity. Often the concept of positive health is lacking, the aim merely coping with tasks, avoiding symptoms and perhaps adding a bit of tat glamour. Unsurprisingly, they become less able, less attractive and unthinking in many ways, and seem unworthy of social benefits. They too have industries that cater to and often increase their needs - deceptive advertising, rubbish food, inferior shops, incredibly expensive loans, shoddy entertainment, even fashions like tattooing and grunge that, unintended, endorse damage. With no economic security they become deskilled, disordered scroungers. With little self-worth, they assert remnants of status defensively and incline to magical beliefs in lotteries and in useless panaceas, but die earlier. They are hard to help to change and can't avoid that their children will be like themselves. If they want to escape their plight they find inadequate services that are being forced toward perfunctory outcomes.
Positive health extends beyond the physical self and embraces empathy, compassion and morality. Other people are the major sources of stress and danger or friendship and fulfilment. The pathological division in our society swamps efforts to create a healthy and purposeful community.
Edwin Alan Salter PhD
King’s Lynn
Comments:
-
No Article Comments available