Positive Health Online
Your Country

![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
Chronic Fatigue Syndrome and NADH
listed in cfs me long covid, originally published in issue 50 - March 2000
"This is serious," our news anchor told me privately. "You're starting to repeat yourself all the time. People are noticing. I'm worried about you."
"I'm just so busy that I'm forgetting stuff," I told her. I didn't bring up the swollen glands, the unbearable headaches that no medicine could help, and the pain in my joints, which was so intense that I'd often wrap bandages around my wrists and ankles at night to keep them from moving. I was trying to look and act like the old Tim. Everything was just fine. That was what I wanted everyone, especially myself to believe.[1]
The worst was to come. Tim was yet to realise that he would suffer interminably from exhaustion, losing his intellectual capacity, career as a news director, social life, friends, self-esteem and his favourite recreational activity of flying.
He is suffering from an insidiously debilitating and bewildering disease called Chronic Fatigue Syndrome (CFS), which is beyond the comprehension of many people. The disease varies itself in intensity and duration, and is characterised by fatigue, muscular aches and pains, headaches, weakness, sore throats, swelling, depression, fever, sleep disturbances and tenderness in the lymph nodes.[2-4]
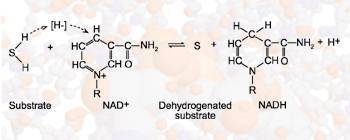
General reaction showing how NAD+ acts as a coenzyme in enzymatic dehydrogenation reactions
CFS is not a new disease and references to similar conditions go back to the 1860s under the names of "Neuromyasthemia", "Yuppie Flu", "Post Viral Fatigue Syndrome", "Chronic Immune Deficiency Syndrome", and "Myalgic Encephalomyelitis". Others such as "Iceland Disease", "Royal Free Disease", "Tapanui flu" and "Akureyri Disease" are named after locations where large-scale outbreaks of the disease occurred. All of these conditions are symptoms of underlying causes, which have not yet been fully identified, and the preferred name is Chronic Fatigue Syndrome because it characterises the major symptom of the illness without referring to aetiology.
Just as Tim was initially in denial of his illness, many doctors suffer from the same problem. They refuse to recognise the condition as they can't find anything physically wrong, and the diagnosis usually given is psychological in nature. However, the facts are that 150,000 people in Great Britain suffer from CFS, including an estimated 24,000 children and young adults, with many more cases going undiagnosed. Younger patients suffer greatly because of the impact that the illness has upon school attendance, compounded by the lack of understanding amongst teachers, educational psychologists, and social workers who seem to attribute the problem to family dysfunction. The incidence of CFS is three times higher in females than males, but can affect people of all ages, races and socio-economic background.[5]
The increasing numbers of people suffering from chronic fatigue, pressure groups, and the mass amount of research data have forced the Centre for Disease Control to produce an operational definition for the diagnosis of CFS based upon clinical symptomatology and exclusion of other physical and psychological diseases associated with fatigue. The main criterion for the disease is unexplained, debilitating fatigue of at least six months' duration, along with four or more symptoms, some of which include neurocognitive dysfunction, myalgias, sore throat, post-exertion malaise and joint pain.[6]
CFS is therefore a clinically defined condition, but there is still little scientific proof due to the lack of definitive laboratory tests. Dr Costa's study investigating the blood flow to the brain of patients with CFS may eventually be used as a scientific, proven diagnostic test. He measures blood perfusion by the 'Single Photon Emission Tomography' (SPET) scan, which shows a reduced blood flow to the brain in patients with CFS. Measures taken to improve blood circulation may improve the mental confusion and exhaustion prevalent in all those suffering.[7]

NADH within the cell
Molecular model of NADH
The research on individual and multifactorial causes of CFS seems endless, as any underlying factors impacting energy levels need to be considered.
The main areas of research focus on the major factors of viruses, low immunity, stress, depression, impaired liver function, environmental illness, iatragenic co-factors, mitochondrial abnormalities and hypothalamus pituitary adrenal axis. Other factors to consider are Candida albicans, leaky gut, hypothyroid, hypoglycaemia, anaemia, nutritional deficiencies, food allergies, sleep disturbances, emotional problems, breathing, posture and lack of exercise.
Focusing on the main areas of research, the underlying viral aetiology of the condition is well established, although there are different views as to the viruses responsible. The British favour enteroviruses such as coxackievirus, ECHO virus and polio virus, and the Americans favour the Epstein Barr virus, including Herpes simplex, cytomegalovirus and Varicella zoster.[8-10] There is also a retrovirus connection, which was discovered by researchers at the Wistar Institute in 1990 who found a possible link between CFS and Human T Cell Lymphotropic Virus 2 (HTLV). Retroviruses are associated with certain leukaemias, lymphomas and chronic diseases of the central nervous system.[11],[12] All of these viruses have the ability to remain dormant in the body, after the initial infection, ready to proliferate when the immune system is compromised.
Immune system abnormalities are therefore associated with CFS.[13]
* Elevated levels of antibodies to viral proteins;
* Decreased natural killer cell activity;
* Low or elevated antibody levels;
* Increased or decreased levels of circulating immune complexes;
* Increased interleukin 2 levels;
* Increased or decreased interferon levels;
* Altered helper/suppressor T cell ratio.
Researchers hypothesise that certain components of the immune system in patients with CFS may be overactive, underactive or both.
The most consistent abnormality is a decreased number or activity of natural killer cells, which can destroy cancer and viral cells.[14] There could also be a reduced ability of the lymphocytes to function, possibly resulting from an altered production of interferon levels, which helps the differentiation and proliferation of the lymphocytes. When interferon levels are low, viral infection is likely and when interferon levels are high, the symptoms are the same as CFS and include memory deficits, muscle aches and lethargy. Similar effects can occur with increased amounts of interleukin 2. Low levels of specific immunoglobulins are also reported, which are closely associated with allergies and the presence of elevated antibodies to viral proteins.[15-22]
An interesting area of research is the impaired activation of the hypothalamic-pituitary-adrenal axis (HPA), which is the hormonal centre of stress control. Demitrack reached this conclusion when he found that CFS sufferers had a reduced production of the adrenal hormone cortisol. Many sufferers do recall a critical period of stress before they developed the symptoms of chronic fatigue. Low cortisol production leads to debilitating fatigue, especially after exercise, joint and muscle pain, enlarged lymph nodes, exacerbation of allergic responses, and disturbances of mood and sleep. This research also connects well with Dr Costa's study and the immune system studies. Linked to stress is depression, which is said to be the commonest cause of chronic fatigue in the absence of any pre-existing physical condition.[23]
Energy is produced in the mitochondria of each cell and therefore changes in mitochondrial function will also contribute to chronic fatigue. These changes can be due to deficiencies in amino acids, enzymes, minerals and vitamins, particularly B vitamins. In one study, CFS patients showed increased 2'-5' A synthetase and RNAse L activity, leading to a depletion of cellular ATP, the energy molecule.[24]
Also indicated in CFS are iatragenic co-factors including prescription drugs: antihypertensives, anti-inflammatories, birth control pills, antihistamines, corticosteroids, tranquillisers, steroids and antibiotics in particular. Antibiotics may be lethal as they can last in the body for up to eighteen months, and are capable of affecting DNA if given for longer than two weeks. They also have a role to play in Candida albicans, leaky gut and allergies, causing weaknesses in the body.
There are close connections between CFS, fibromyalgia and multiple chemical sensitivities.[25-27] The only difference in diagnostic criteria between CFS and fibromyalgia is the requirement of musculoskeletal pain in fibromyalgia, and chronic fatigue in CFS. A person suffering from multiple chemical sensitivity can also display all the symptoms of CFS and fibromyalgia. There are approximately 70,000 chemical compounds (zenobiotics) in current commercial production occurring in food, air, water and pharmaceuticals. Single, multiple, or combinations of these chemicals play havoc in the body and can react with chromosomes in our cells to cause damage to DNA. One example is the chemical used in sheep dips, which causes organophosphorous pesticide poisoning resulting in similar symptoms to CFS and fibromyalgia.[28] Most of these chemicals are fat-soluble and the enzymes for the Phase 1 and Phase 2 liver detoxification pathways are responsible for breaking down these toxins for easier elimination to the digestive tract, via the gall bladder. However, if the liver enzymes are not functioning, the toxins will be stored in the body's cells, particularly in the adipose tissue. Fevers or fasting may result in the release of large quantities of these fat-soluble pollutants from the storage sites into the system, thus causing toxic poisoning. This could account for the high incidence of chronic fatigue onset after fevers.[29] If a person is affected by chemicals it may be wise to give the liver support through foods, supplements and cleansing diets.
Simplified diagram of the stages of metabolism that lead from food to NADH.
This series of reactions produces ATP, which is then used to drive biosynthetic reactions
and other energy-requiring processes in the cell
Successful treatment of CFS requires comprehensive diagnosis, taking into account medical history and a study of the body's systems. The procedure involves eliminating the elements causing fatigue, and will include the major factors we have discussed, as well as checking for other factors such as Candida albicans, leaky gut, hypothyroid, hypoglycaemia, anaemia, nutritional deficiencies, food allergies, sleep disturbances, emotional problems, breathing, posture and lack of exercise. Appropriate treatment can then be given for the person with CFS based on their biochemical individuality.
A good starting point for any CFS sufferer would be to look at their diet, as energy levels are directly related to nutrient intake. It is recommended that the patient follows a well-balanced, organic, wholefood nutrition programme, high in fresh foods and vegetables containing soluble and insoluble fibres, and low in saturated fat and salt. Lots of filtered water should also be taken. This will help to cleanse the body of its toxic overload and avoid further damage from the chemicals found in processed foods and drink.
Useful foods to include are the Omega 3 and Omega 6 fatty acids found in flaxseed and fish oils, which enhance the immune system,[30] as well as garlic containing allicin, which has potent antibacterial, antifungal, anti-inflammatory, antiviral, anti-tumour and antiparasitic properties.[31]
Supplementation is also important, as almost any nutritional deficiency will result in chronic fatigue. Amongst the important ones that enhance the immune system are beta carotene, retinol, pantothenic acid, pyridoxine, riboflavin, D-alpha tocopherol, ascorbic acid and cobalamin, along with adaptogenic plants such as Astragalus membranaceus (Astragalus) and Eleutherococcus senticosus (Siberian Ginseng).[32]
Glycyrrhiza glabra also has anti-viral properties and a role to play in the HPA axis as it increases cortisol levels by blocking the enzyme that breaks it down. The whole root must be used as deglycyrrhizinated acid (DGL) has had the glucocorticoid- potentiating glycyrrhizic and glycyrrhetinic acids removed.[33],[34]
Supplements specifically involved in fatigue are iron, folic acid, B vitamins and magnesium. Magnesium is needed to produce ATP (energy) and it does this in two ways. In the aspartate form, it feeds into the Krebs cycle to provide ATP and in the citrate form, it is a component of the Krebs cycle.[35] CoQ10 (Ubiquuinone) is a co-factor in the electron transport chain in the mitochondria involved in the synthesis of ATP (energy), and is essential for the health of the tissues and organs.
Research continues to help those suffering from this clinically perplexing disorder and a new supplement called NADH offers new hope for CFS. Stabilised, oral NADH has been developed by Professor George D Birkmayer, MD PhD. and was patented in 1993. NADH is the biological substance nicotinamide adenine dinucleotide, which is a metabolyte of niacinamide, the active co-enzyme form of vitamin B3.[36]
It is an important molecule for producing energy in the body as it is the main carrier of electrons during the oxidation of macronutrients, which produce energy in the mitochondria of each cell. Each molecule of NADH can produce three molecules of adenosine triphosphate (ATP), the energy compound. (see diagram above).
All cells contain NADH; the quantity is dependent on the amount of energy that the cell requires. For example, the heart muscle, which has to contract 86,400 times a day, needs 90 milligrams and the brain and muscle tissue 50 milligrams. The more NADH the cell has available the more energy it can produce, and it is therefore an invaluable supplement for CFS. However, as NADH is a co-enzyme (helper enzyme), it is also able to amplify other enzymes to be catalysts in many different biochemical reactions within the body, thereby helping other factors involved in CFS. It aids immunity by being involved in the formation of reduced glutathione, the cell's major antioxidant, to prevent free radical attack. Reduced glutathione, in turn, provides further support for the immune system by regenerating the vitamin antioxidants C and E.[38] NADH also helps to repair DNA damage, preventing detrimental changes on a cellular level, and aids in the production of dopamine, adrenalin and seratonin to lift depression, aid co-ordination and improve mental function.[39-41]
An approved FDA ongoing study, which started in 1996, is being conducted by Georgetown University to evaluate the efficacy of NADH, administered orally to a group of patients with CFS, in a double-blind, placebo-controlled, crossover study. The 26 patients who fulfilled the Centre for Disease Control's criteria for CFS completed the study. Medical history, physical examination, laboratory studies and a questionnaire were obtained at weeks 4, 8 and 12. The subjects received either 10mg of NADH or a placebo for four weeks and then had a four-week break before taking the alternate regimen for a further four weeks.
The results showed that 31% of the patients responded favourably to NADH and that there were no side effects. A further open label follow up study revealed a 72% improvement. The main response of the patients was characterised by improvement in fatigue, a decrease in symptoms and improvement in the quality of life.[42]
In the follow up study, Dr Bellanti at the American College of Allergy, Asthma and Immunology found that 75% of the patients showed elevated levels of 5-HIAA, the major breakdown product of seratonin, which is involved in brain chemistry. When treated with NADH, 70% of the patients returned to a normal range. These results suggest that the measurements of urinary 5-HIAA may be a useful predictive marker of disease activity in CFS patients, and could also provide an objective measure of improvement following therapy with NADH.[43] The results of these studies clearly indicate that NADH may be a valuable adjunctive therapy in the management of CFS.
CFS is real, elusive and here to stay. There is no one specific treatment, nutrient or cure available. To overcome the disease, the methodology has to be supportive of the individual's physiological and psychological needs, and a regime of balancing and pacing rest and activity must be followed to initiate the body's own exquisite healing mechanisms.
References
1. Timothy Kenny. Extract from Living with Chronic Fatigue. Thunder's Mouth Press. 1994. ISBN 1-56025-075-5.
2. Fukuda K, Straus SE, Hickie I et al. Chronic fatigue syndrome: A comprehensive approach to its definition and study. Ann Inter. Med. 121: 953-959. 1994.
3. Komaroff AL, Buchwald DS. Chronic fatigue syndrome: An update. Ann Rev Med. 49: 1-13. 1998.
4. Sharpe MC, Archard LC, Banatvala JE et al. A report chronic fatigue syndrome: Guidelines for research. JR Soc Med. 84: 118-121. 1991.
5. National Institutes of Health Medicine for the Public. Chronic Fatigue Syndrome. NIH Publication. 90: 3059. 1990.
6. Holmes GP et al. CFS: A working case definition. Ann Intern Med. 108: 387-389. 1998.
7. Costa DC et al. Postviral Fatigue Syndrome. Brit Med Journal. 304: 1567. 1992.
Costa DC et al. Brainstem perfusion is impaired in Chronic Fatigue Syndrome. QJM 88(11): 767-73. Nov 1995.
8. Jones JF, Ray C, Minnich L et al. Evidence for active Epstein Barr virus infection in patients with persistent unexplained illness: Elevated anti-early antigen antibodies. Ann Intern Med. 102: 1-7. 1985.
9. Sumaya CV. Serological and virologic epidemiology of Epstein Barr virus: Relevance to chronic fatigue syndrome. Rev Infect Dis. 13 (suppl): 19-25. 1991.
10. Drake DC. CFS AIDS type virus link. The Philadelphia Inquirer. September 1990.
11. Wistar Institute Philadelphia, PA. September 4 1990.
12. Komaroff AL. Chronic Fatigue syndrome: Relationship to chronic viral infections. J Virol Meth. 21: 3-10. 1988.
13. Pizzorno Jr J and Murray M. Textbook of Natural Medicine. Harcourt Brace and Company Ltd. p.427. ISBN 0-443-05945-4. 1999.
14. Caligiuri M, Murray C, Buchwald D et al. Phenotypic and functional deficiency of natural killer cells in patients with chronic fatigue syndrome. J Immunol 139: 3306-3313. 1987.
15. Gupta S. Vayauvegula B. A comprehensive Immunological analysis in chronic fatigue syndrome. Scand J Immunol. 33: 319-327. 1991.
16. Lloyd A, Hickie I, Wakefield D et al. A double blind placebo controlled trial of intravenous immunoglobulin therapy in patients with chronic fatigue syndrome. American J Med. 89: 562-568. 1990.
17. Buchwald D, Komaroff AL. Review laboratory findings for patients with chronic fatigue syndrome. Re. Infect Dis. 13 (suppl): 12-18. 1991.
18. Klimas NG, Fernando FR, Morgan F and Fletcher MA. Immunologic abnormalities in chronic fatigue syndrome. J Clin Microbiol. 28: 1403-1410. 1990.
19. Mawle AC, Nisenbaum R, Dobbins JG et al. Immune responses associated with chronic fatigue syndrome: A case controlled study. J Infec. Dis. 136-141. 1997.
20. Bellanti JA, Forsyth LM, MacDowell, AL and Preuss HG. Chronic Fatigue Syndrome: unravelling a new dilemma. J Am College Nutr. 1998.
21. Strauss SE, Dale JK, Wright R and Metcalfe DD. Allergy and the chronic fatigue syndrome. J Allergy Immunol. 81: 791-795. 1998.
22. Demitrack MA et al. Evidence for impaired activation of the hypothalmic- pituitary-adrenal axis in patients with chronic fatigue sundrome. J Clin Endocrinol and Metab. 73: 1224-1234. 1991.
23. Lloyd A, Hickie C et al. Cell mediated immunity in patients with chronic fatigue syndrome, healthy control subjects and patients with major depression. Clin Exp Immunol. 87: 76-79. 1992.
24. Sudadolnik RJ, Reichenbach NK, Hitzges P et al. Upregulation of the 2-5 A synthetase/Rnase L antiviral pathway associated with chronic fatigue syndrome. Clin Infect Dis. 18 (suppl): 96-104. 1994.
25. Buchwald D and Garrity DL. Comparison of patients with chronic fatigue syndrome, fibromyalgia and multiple chemical sensitivities. Arch Int Med. 154: 2049-2053. 1994.
26. Komaroff AI and Goldenberg D. The chronic fatigue syndrome. Definition, current studies and lessons for fibromyalgia research. J Rheumatol. 16: 23-27. 1989.
27. Hughes Jr, Higgins ST, Bickel WK et al. Caffeine, coffee and the medical consequences. West J Med. 157: 544-553. 1992.
28. Rae W. Chemical Sensitivity vols. 1-4. Lewis Publishers. Boca Raton. 1992.
29. Corrigan F. Pesticide exposure, fatigue and GABA receptor sensitivity. Lochgilphead Hospital. Scotland. 1994.
30. Hind A. Nutrients as Modulators of Immune Function. J of Nutrition. 122 (3): 610. 1992.
31. Sharma VD, Sethi MS, Kumar A et al. Antibacterial property of Allium sativum Linn. In vivo and in vitro studies. Ind J Exp Biol. 15: 466-468. 1977.
32. Bohn B, Nebe CT and Birr C. Flow cytometric studies with Eleutherococcus senticosus extract as an immunomodulatory agent. Arzniem Forsch. 37: 1193-1196. 1987.
33. Baschetti R. Chronic fatigue syndrome and liquorice. New Zealand Med J. 108: 156-158. 1995.
34. Brown D. Licorice root – potential early intervention for chronic fatigue syndrome. Quart Rev Nat Med. 95-96. Summer 1996.
35. Cox IM, Campbell MJ and Dowson D. Red blood cell magnesium and chronic fatigue syndrome. Lancet 337: 757-760. 1991.
36. Gilham B, Despo K, Papachristodoulou J. Hywell Thomas Wills' Biochemical Basis of Medicine 3rd Edition. Reed Educational and Professional Publishing Ltd. ISBN 0-7506-2013-7. 1997.
37. Prof G Birkmayer MD. NADH: The Energising Co-enzyme PhD. Keats Publishing Inc. ISBN 0-87983-863-0. 1998.
38. Demopoulos HB et al. The possible role of free radical reactions in carcinogenesis. J Environ Path Tox. 3: 273-303. 1980.
39. Birkmayer JGD, Vrecko C, Vole D and Birkmayer W. NADH- New therapeutic approach to Parkinson's disease, comparison of oral and parenteral application. Acta Neurol Scand. 87 (Suppl) 146: 32-35. 1993.
40. Birkmayer JGD. Coenzyme NADH: New therapeutic approach for improving dementia of the Alzheimer type. Ann Clin Lab Sci. 26: 1-9. 1996.
41. Birkmayer JD and Birkmayer W. The co-enzyme NADH as biological antidepressive agent experience with 205 patients. New Trend in Clin Neuropharm. 5: 75-78. 1991.
42. Bellanti JA, Forsyth, LM, MacDowell-Carneiro AL, Birkmayer GD and Preuss HG. NADH and chronic fatigue syndrome: A new therapeutic approach (abstract). Ann Allergy Asthma Immunol. 80-82. 1998.
43. Forsyth LM, MacDowell-Carneiro AL, Birkmayer GD et al. The measurement of 5-HIAA urinary concentrations as a predictive marker of efficacy of NADH in chronic fatigue syndrome (manuscript in preparation). 1998.
Further Information
NADH can be obtained from the Nutri Centre in London and can be ordered by telephone on 020-7436 5122 or by post to The Nutri Centre Ltd, Freepost 26 Lon 14028, London WIE 3DR.
Comments:
-
No Article Comments available