Positive Health Online
Your Country

![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
A Beginner’s Guide to ME/CFS: Myalgic Encephalomyelitis, by So Many Names - Part I
listed in cfs me long covid, originally published in issue 199 - October 2012
A Beginner’s Guide to ME/CFS is the title of a little book by myself which includes essential information and recommendations from Dr. Leslie O. Simpson, which will be available on Amazon Kindle by the time this article appears. Our aim is to demystify this illness, present the simple principles which need to be taken on board by sufferers and carers (as well as our doctors, and our medical services, not to mention the media and the general public). This article, written in two parts, to be concluded in Issue 204, summarizes some of what we have to say.
To you, the patient: Right now, you are sick. But you know, and I know who you are, beyond this illness. You are energetic, conscientious, ambitious, you always go the extra mile. You have high standards for yourself in everything you do. When you get sick, which isn’t very often, you still do all you can to meet your commitments. You have interests that you are excited about; you enjoy your family and friends. If you have been criticized in the past, the ‘criticisms’ are most likely to have been expressions of concern - that you do too much, you put others first, you don’t take care of yourself - never that you are lazy, or don’t pull your weight.
So when this illness comes out of the blue, it is totally alien to the kind of person that you are. When you find yourself just going limp, for no obvious reason, and it goes on and goes on, you feel more than just sick. You are losing not just the activities you used to do - you may be threatened about losing your job, your income, with all that that would mean, or you find yourself unable to take proper care of your children. Your family or partner may even be sceptical and unhelpful, believing it is best to tell you to ‘pull yourself together’. (You only wish you could!) And if they are sympathetic and helpful, you feel terribly guilty about being a burden, more so because there is no visible reason for your being so incapacitated.
But, even more disturbingly, this illness forces you to change your way of living to such a degree that you may even feel you are losing your sense of your identity - the person you have always believed yourself to be, the person you want to continue to be. That is the most profound psychological challenge of all.
What about treatment? Here is the wisdom of the doctors who originally spent years studying this illness, and the course of this illness for hundreds of patients, over the years:
Sir Donald Acheson, former UK Chief Medical Officer, wrote about ME/CFS:
‘In the management of the acute phase, absolute rest provides the best outcome’ and
‘the association of premature attempts at rehabilitation with relapse are well described.’[1]
While Dr. Melvin Ramsay, the Consultant in Infectious Diseases who spent his whole career after the 1955 Royal Free Hospital outbreak studying this illness warns:
“...in those patients whose dynamic or conscientious temperament urge them to continue efforts despite profound malaise or in those who, on the false assumption of ‘neurosis’ have been exhorted to ‘snap out of it’ and ‘take plenty of exercise’ the condition finally results in a state of constant exhaustion.”
and
“the degree of physical incapacity varies greatly, but the dominant clinical feature of profound fatigue is directly related to the length of time the patient persists in physical effort after its onset; put in another way, those patients who are given a period of enforced rest from the onset have the best prognosis.”[2]
In simple terms, the best prescription, as soon as you suspect that you might have ME, is complete rest. And over the long term, conserving the use of your muscles as much as possible, by gratefully accepting help from others, using every labour-saving device you can afford, even a simple thing like always keeping your head supported - keep your energy for absolutely necessary tasks, a bit for doing something you enjoy, and keep a balance for your body to apply to the process of recovering.
Trials are afoot for drugs that can help, and Rituximab (normally used for the treatment of non-Hodgkins lymphoma) has cured enough people in Norway, that the government has apologized to patients who have been told it was a ‘behavioural’ problem and treated with Cognitive Behaviour Therapy (CBT) and Graded Exercise Therapy (GET). They now recommend against these treatments.[3]
Predictably, this important information has been virtually ignored by the UK media, apart from an article in the New Scientist.[4] Likewise, the Invest in ME Conference, held on 1 June, 2012, in London was unreported in the UK, despite invitations to journalists.
However the view that ME is a psychiatric (‘somatoform’) disorder, best treated with CBT and GET is incorporated into the UK’s NICE Guidelines[5] and into the practice of many, if not most, of our Specialist Treatment Centres,[6] which means that we are being offered treatments which at best are unhelpful and most probably, will make us worse.
Rituximab, and other drugs which are being trialled, are very expensive, and not likely to become generally available for a long time.
However, the research of Dr. Les Simpson into the effect of easily available supplements to improve blood flow does offer us the possibility of significant improvement in our well-being.
To put it very briefly, many chronic conditions, including ME, involve changes in our red blood cells. Usually the vast majority of these are biconcave discocytes - flat, circular, with an indentation on each side. Red blood cells in this shape can curl up (deform) enough to travel through the tiniest of our blood vessels, the capillaries, which serve every cell in our body by delivering oxygen and removing waste substances. You are probably familiar with the fact that blood goes from the heart to our lungs, where the red blood cells absorb oxygen, which is then circulated through our arteries and into the smaller blood vessels, the capillaries. The oxygen is delivered to our cells, waste products removed. Then our red blood cells return to our heart via the veins, to be sent to the lungs to discharge carbon dioxide and collect more oxygen, repeating the whole cycle.
In our muscles, this whole process is the aerobic (oxygen-using) metabolism, and when it is working properly, aerobic exercise will be good for us, encouraging the muscles to gain strength, and providing many other health benefits. When further exertion causes the muscles’ need for oxygen to become greater than the blood’s ability to provide it, there is a shift into what is called the anaerobic metabolism. The anaerobic metabolism is available to us for emergencies, life-threatening situations in which we need that burst of super-strength. Our marathon runners, our weight-lifters, any athletes engaged in extreme muscular exertion, are making use of the anaerobic metabolic system, which is only designed to cope for a short time. For those of us who are not in training, the experience of day-after fatigue and cramps, after an unplanned tennis game, long hike, or bout of serious gardening is probably quite familiar! This is the after-effect of our use of the anaerobic metabolism in muscles inadequately prepared for extra exertion.
This potential for doing oneself some harm is the reason for all those directions about carefully warming up before and cooling down after more strenuous exercise, and building up strength through aerobic exercise before undertaking physical challenges such as running a marathon.
But the possibility for building up muscular strength through exercise relies on the normal, efficient functioning of the aerobic metabolism, and this in turn relies on the ability of our red blood cells to flow easily through our circulation, including capillaries which may be as narrow as half their circumference. For blood flow to be normal, they have to be flexible (deformable) enough to do that.
Les Simpson’s research (the name of his subject is ‘hemorrheology’, and for reasons unknown, it is not included in medical textbooks or the general knowledge of doctors) into the shape and behaviour of the red blood cells demonstrates that even in the blood of healthy people, there are a variety of other shapes which these cells can assume - he identifies six. The cells which do not have the biconcave discocyte shape are relatively inflexible (non-deformable), and can slow down or even block the travel of blood through the smallest capillaries. But in healthy people, these irregular shapes are relatively infrequent.
However, his study of micrographs of immediately-fixed samples of blood show that in many chronic conditions, the red blood cell population contains a much higher proportion of the irregularly shaped cells, and the circulation of blood through the capillaries becomes much less effective. (One way of describing this situation is that blood becomes thicker.)
We know that specific areas of the body and brain are particularly vulnerable to the resulting shortage of oxygen and build-up of waste products (oxidative and nitrosative stress). These include the muscles, the cognitive areas of the brain, and the endocrine system which regulates various bodily functions. (This provides an elegant explanation for the range of apparently unrelated symptoms which are typical of ME.)
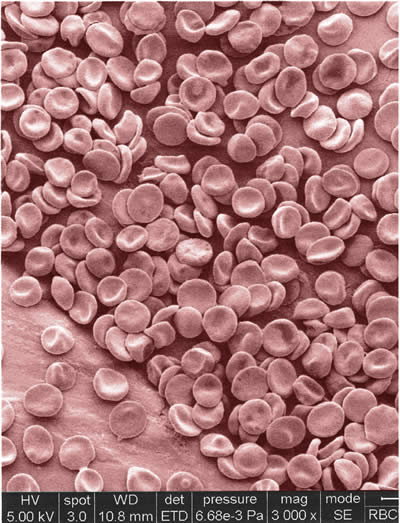
Photo is one of a set made from a sample of the author's
blood, immediately fixed, micrograph dated 8/7/2010. The author has
had ME since 1986; Dr Les Simpson said that the shape populations
were consistent with chronic ME. Micrographs taken by David,
McCarthy, Experimental Officer, Electron Microscopy Unit, The School
of Pharmacy, University of London. (David.McCarthy@pharmacy.ac.uk)
In ME, this is the mechanism which interferes with the normal functioning of our aerobic metabolism and explains why our anaerobic metabolism comes into play much sooner than in healthy individuals. A defining symptom of ME is delayed and protracted fatigue, requiring a much longer than normal time for recovery. This is the kind of reaction to be expected as a result of overuse of the anaerobic metabolism, and explains why we who have ME begin to experience muscle weakness, muscle failure, and the threat of ongoing pain after even the slightest exertion. Further exertion, as described so well by Acheson and Ramsay, will result in greater and longer-lasting exhaustion.
Les’s research also shows that supplements which improve blood flow will improve our well-being, and suggests we make a trial first of 4 g of Genuine Evening Primrose Oil (so choose your source carefully) for six weeks. If no benefit is experienced, then go on to 6g of fish oil (not fish liver oil) per day for six weeks. Further possibilities would be vitamin B12 as hydroxocobalamin, or pentoxyfilline. A significant percentage of people who have ME will benefit from one or another of these supplements.
Les does not suggest that these will address the original causes of ME, which remain matters under research, or provide a cure, only that they can offer significant improvement in many cases.
Some Useful Websites
National Alliance for Myalgic Encephalomyelitis www.name-us.org includes definitions and articles from the earliest researchers – Ramsay, Acheson, Dowsett.
One Click www.theoneclickgroup.co.uk Put ME/CFS into their search engine to find an article ‘Mobilising ME/CFS Charities to Smash Flawed PACE Trial Results, by Lara Hessler, 14/4/2011. This explains the changes to the disability assessment system as of that time (there are further changes taking place at the moment – August 2012). Her suggestion is that ME Charities should pay for individual patients to have medical tests (not allowed by the NICE Guidelines) to prove that they are not suffering from ME/CFS as defined by PACE, but have a biologically-based condition.
You can access the full text of the Myalgic Encephalomyelitis: International Consensus Criteria by putting this into their search line and clicking onto the Google reference, which will bring up a page on it, go to the bottom of the page and click onto ‘Full Text’.
For a very scientific explanation of why CBT and GET are harmful, go onto One Click, and type in ‘Twisk and Maes’.
Invest in ME, www.investinme.org provides reports on research and on their annual conferences. This is the source of the information about development in Norway – the Rituximab trials, in which some patients have been cured. These have resulted in a government apology to people with ME/CFS who have been told their illness was a ‘behavioural’ problem, and treated with CBT and GET.
ME-CFSCommunity, at www.me-cfscommunity.com , or www.cfsknowledgecenter.ning.com will take you to a very helpful site for the most recent research, with comments by the moderator. Also there are some good forums for special topics, and you can join chat groups.
IACFSME www.iacfsme.org This is a U.S. based site, which is announcing the formation of a new journal, also they take a definite stand against the proposal to label ME a psychiatric problem in DSM V.
MEActionUK, at www.meactionuk.org/ or on Facebook, MEActionUK, www.facebook.com/pages/MEActionUK/287426748781 Useful for following the politics and medical politics of ME.
Bibliography
1. Acheson AD. The clinical syndrome variously called behign myalgic encephalomyelitis, Iceland Disease and epidemic neuromyasthenia. [book auth.] Byron M Hyde and J A Goldstein. The Clinical and Scientific Basis of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. s.l. : The Nightingale Foundation 'In the management of the acute phase, absolute rest provides the best outcome' 'The association of premature rehabilitation with relapse is well described'. 1992.
2. Ramsay MA. Myalgic Encephalomyelitis: A Baffling Syndrome With a Tragic Aftermath. National Alliance for Myalgic Encephalomyelitis. Contains quotes re rest best treatment, incapacity directly related to continued exertion. [Online] www.name-us.org/Definitions Pages/DefRamsay.htm . Myalgic Encephalomyelitis. 1986. [Cited: 6 September 2012.]
3. The Drug and the Possibility of Changing Everything. Jelstad, Jorgen. 1, s.l. : Invest in ME. Journal of IiME, Vol. 6, pp. 13-17. Page 16 Norwegian Gov't apologises to ME patients for treating ME as a 'behavioral' problem, recommends against CBT and GET. May 2012.
4. Chronic fatigue syndrome eased by cancer drug. Coghlan Andy. 2836. New Scientist. Small article, significance in challenging the Wessely School beliefs not recognised/developed. 26 October 2011.
5. NHS National Institute for Health and Clinical Excellence. CG53 Chronic Fatigue, Myalgic Encephalomyelitis. www.nice.org.uk . Emphasis is on 'maintaining and if possible, gradually extending an individual's physical capacity'. [Online] August 2007. [Cited: 3 August 2012.]
6. ME Association. NHS specialist services throughout the UK. ME Association. Provides staff lists :Mostly psychiatrists, psychologists, OT's, Physio's, Rehab. www.meassocition.org.uk/?page_id+1382 [Online] [Cited: 10 August 2012.]
7. Spotila, Jennie. Exercise Testing and Results. Occupy CFS. [Online] Occupy CFS. Gives a very detailed explanation of the role of reaching/exceeding anaerobic threshold in ME/CFS. http://www.occupycfs.com/exercise-testing-and-results/comment-2032. 3 July 2012. [Cited: 5 September 2012.]
8. Causes of Death Among Patients With Chronic Fatigue Syndrome. Jason LA, Corradi K, Gress S, Williams S, Torres-Harding S. 7, s.l. : Taylor & Francis Online. Health Care for Women International, Vol. 27, pp. 615-626. Main causes of death: heart failure (30 yrs younger than av), cancer, suicide, 10 years younger than av. 2006.
To be Continued in Issue 204
Comments:
-
Graham Watsom said..
An excellently written article, providing useful, up-to-date information for the CFS/ME sufferer.
-
Graham Watson said..
It is interesting to note that treatments claiming success over CFS/ME are largely based around NLP, but the author herself is an accredited NLP psychotherapist and has not been able to rid herself of the illness(nor does she make any claims that it is helpful).
The choice of words in the 'About Nancy Blake' is also interesting; 'Recovering from M.E. since 1986....' This is an extremely slow recovery,isn't it? Doesn't sound like recovery to me at all. This sounds like terminology from Alcoholics Anonymous (used by people who don't drink any more) or .... NLP or CBT. Let's call a spade a spade or we'll get nowhere with this extremely debilitating illness. Imagine going the doctor and saying, 'I'm recovering from CFS, can you help me?' Most people with CFS are not recovering at all, but they certainly are suffering. Why not just say so?
-
Nancy Blake (author reply) said..
Graham, thanks so much for your positive comments! It is right that 'recovery' is rare, and considerably more rare as CBT and GET are used as treatments. In the days when people were hospitalised and did rest (e.g. hospitalisation meant rest, not being bullied by staff determined to force the patient to exert him/herself), recovery seems to have happened much more often. When a treatment agency gives the impression that the goal of treatment is to get the person able to climb mountains and run marathons, I would feel extremely wary, to put it mildly. NLP does not address the causes of ME, and the misuse of NLP to treat ME seems to me likely to be harmful, as I understand some patients have found.
However when I describe myself as 'recovering from' ME, that is based on NLP. I don't want to 'have' ME, and I don't want to be 'suffering from' ME, and I am not going to falsely describe myself as 'recovered from ME' because although when I started I could hardly cross a room, and now I teach piano, work as a psychotherapist, write, drive, do errands, but still have to be careful not to get overenthusiastic about activity, it is accurate (as well as psychologically sound) to use the expression 'recovering from'. Except perhaps that that implies I will reach complete recovery at some point, and as for most people who have this illness, that is unlikely. (And I hope I've made the point that going to a doctor about ME or CFS, whatever you say about it, is unlikely to be helpful - whether your doctor is sympathetic or skeptical, the Guidelines available to them from NICE are not helpful!)
-
Graham Watson said..
Nancy, Thanks very much for your comprehensive response to my comments.
-
Lynn Chinnock said..
I have suffered from M.E since 1992, I am lucky that I go to a special unit at my local health clinic which offers help and advice. I think if I had the help in the early stages I might be a lot better now.
My health has deteriorated as I have got older, however, I think what Nancy meant is that you can have a 'good spell' which lasts quite a while. During these 'good spells' you can truly imagine that you are in recovery, and indeed, some people do go on to improve enough to lead a relatively normal life.