Positive Health Online
Your Country

![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Lotus Books]](/img/original/TopicbannerAvatar/953.adb373b0210368e0c9ce4d9a8a9f01aa.jpg "Lotus Books")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
Plantar Fasciitis
by Brian A Rothbart PhD(more info)
listed in bodywork, originally published in issue 174 - September 2010
Stedmens Medical Dictionary defines plantar fasciitis as an inflammation of the plantar fascia, often caused by an overuse mechanism, which results in foot and heel pain.[1] This definition is now thought to be incorrect due to the absence of inflammatory cells within the plantar fascia. Instead, the plantar fasciitis is now thought to be due to a degeneration of the collagen fibres within the plantar ligament resulting from micro trauma.
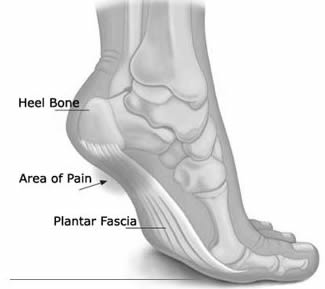
Plantar fasciitis is sometimes incorrectly referred to as a heel spur. A heel spur is a bony turburence (growth) that occurs where the plantar fascia attaches to the calcaneus (heel bone). The heel spur is now thought to be a direct result of a repetitive pulling of the plantar fascia. A heel spur may or may not result in heel pain. Whereas heel pain is always present in plantar fasciitis.
There are other, less common conditions that can result in heel pain:
- Nerve entrapment of the post tibial nerve;
- Stress fracture of the heel bone;
- Necrosis of the fat pad underneath the heel bone;
- Reiter's syndrome;
- Ankylosing spondylitis.
Symptoms of Plantar Fasciitis
The stabbing pain resulting from plantar fasciitis is typically located on the bottom and inside of the heel bone, where the plantar fascia attaches to the heel bone. The pain is usually worse first thing in the morning. After a few steps, the pain eases. However, it may return after long periods of standing or after sitting for long periods of time.The plantar fascia ligament is like a rubber band. It loosens and contracts with movement. The plantar fascia also absorbs weight and pressure as you walk. If the weight and pressure on the plantar fascia is excessive (e.g., excessive running, jumping etc), micro-tears in the collagen fibres within the plantar fascia can occur. This is why athletes are prone to developing this condition.
A contributing factor in the development of plantar fasciitis is walking or exercising in improper shoes (shoes that do not fit correctly, provide inadequate support or cushioning). This can impair the weight distribution through foot which, in turn, can significantly increases the stress on the plantar fascia ligament.
Treating Plantar Fasciitis
The heel pain resulting from plantar fasciitis is often intractable (non responsive) to any one type of therapy. For this reason, many different types of therapy are used to treat this condition:- Apply Ice Packs
Icing will help to diminish some of the symptoms and control the heel pain. Icing is especially helpful after an acute exacerbation of symptoms; - Exercises and Stretches
Exercises and stretches are designed to relax the tissues that surround the heel bone. Some simple exercises, performed in the morning and evening, often help patients feel better quickly; - Anti-Inflammatory Medications
Anti-inflammatory medications help to both control pain and decrease inflammation. Over-the-counter medications are usually sufficient, but prescription options are also available; - Shoe Inserts
Typically these shoe inserts have built in arch supports to take the stretch of the plantar ligament or heel pads to cushion the areas of pain; - Night Splints
This helps prevent the plantar ligament from contracting while you sleep, and hopefully not as painful in the morning.
In 1971, I published a paper in the Journal American Podiatric Association that challenged the then current thought that Plantar Fasciitis was frequently due to a heel spur irritating the long plantar ligament. I suggested that Plantar Fasciitis (heel pain syndrome) was the result of excessive foot twist. My paper was based on my findings that:
- Many of my patients with heel pain (Plantar Fasciitis) did not have heel spurs;
- Many of my patients with heel spurs did not have heel pain;
- All of my patients with heel pain had foot twist.
- Foot twist expands the foot (longer and wider);
- As the foot becomes longer, the long plantar ligament is stretched;
- As the long plantar ligament is stretched, micro tears occur in the attachment of the ligament into the heel bone;
- These micro tears result produce an inflammatory reaction, culminating in heel pain.
However, the question that still needed to be answered was: what causes the foot to twist?
This question was answered in a paper I published in 2002 in the Journal Movement Bodyworks Therapy, in which I linked foot twist to two embryological foot structures, the Rothbarts Foot and the PreClinical Clubfoot Deformity. I theorized that these two foot structures force the foot to twist due to the incomplete osseous development of the calcaneal (heel) and/or talar bones.
Therapy
Traditionally, Plantar Fasciitis is treated with arch supports. The rationale of this therapy is to reduce the stretch on the long plantar ligament (plantar aponeurosis), thereby allowing the inflammation at its insertion points to heel (See Figure 1 below). However, a randomized trial published by Landorf et al (2006) concluded that this approach resulted in only "small reductions in pain for people with Plantar Fasciitis". In my practice, I have found that arch supports frequently increase the pain in patients suffering from Plantar Fasciitis.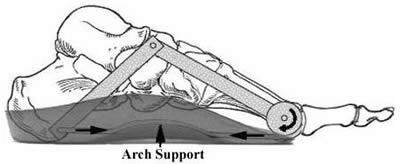
which in turn, predisposes this ligament to further micro tears.
Rothbart Proprioceptive Therapy
Rothbart Proprioceptive Therapy has proven to be very effective in eliminating heel pain associated with Plantar Fasciitis. The reason this therapy is so effective is that it treats the underlying cause of foot twist, which in turn, decreases the elongation of the long plantar ligament (and resulting inflammation of its insertion points as it is being torn away from the bone) (See Figure 2 below).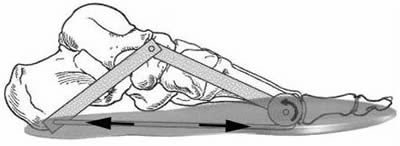
tension on the long plantar ligament (plantar aponeurosis).
Notes and References
1. www.drugs.com/search.php?sources[]dict&specific_search=1&searchterm=plantar+fasciitis&x=0&y=0 Bibliography and Further Reading
Landorf KB, Keenan AM and Herbert RD. Effectiveness of Foot Orthoses to Treat Plantar Fasciitis., 166:1305-1310. 2006.Rothbart BA. Heel spur and heel spur syndrome. Journal American Podiatric Medical Association(JAPMA), 61(5):186-9. 1971.
Rothbart BA. Medial Column Foot Systems: An Innovative Tool for Improving Posture. Journal of Bodywork and Movement Therapies (6)1:37-46. 2002.
Further Information
For more information on Rothbart Proprioceptive Therapy, visit: What is Rothbart Proprioceptive Therapy (http://blog.rothbartsite.com/2009/03/20/what-is-rothbart-proprioceptive-therapy.aspx ).Comments:
-
No Article Comments available
Post Your Comments:
About Brian A Rothbart PhD
Brian A Rothbart DPM PhD ND known as the Father of Chronic Pain Elimination, is one of the top internationally recognized experts in the elimination of chronic back, neck, hip, knee, and foot pain.
With 40 years as a pioneering researcher and physician, Professor Rothbart discovered the previously unknown source of chronic musculoskeletal pain and invented an innovative therapy which eliminates it without the use of drugs or surgery. He has not only eliminated his own chronic musculoskeletal pain, but has helped thousands of others find that same freedom and get their life back.
Professor Rothbart teaches, lectures and has been extensively published in leading medical journals. He is the author of two books: Forever Free From Chronic Pain and The Foot’s Connection to Pain. He has appeared on radio, written a syndicated column and hosted a television show speaking with people worldwide about how to permanently eliminate their chronic musculoskeletal pain. He may be contacted via professorrothbart@gmail.com www.rothbartsite.com/