Positive Health Online
Your Country

![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: http://www.balens.co.uk]](/img/original/BannerAvatar/2148.50367fa908013fae0a7f1a171543ef92.jpg "http://www.balens.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
![[Image: Lotus Books]](/img/original/TopicbannerAvatar/953.adb373b0210368e0c9ce4d9a8a9f01aa.jpg "Lotus Books")
The Plantar Grade Foot vs. Morton’s Foot, Rothbarts Foot and the PreClinical Clubfoot Deformity
by Brian A Rothbart PhD(more info)
listed in bodywork, originally published in issue 291 - January 2024
The foot structure you were born with greatly determines your overall health. For example; a plantar grade foot (what you would think of as being a ‘normal’ foot) is linked to having healthy muscles and joints and overall good health. Whereas 3 other foot structures can cause problems ranging from simple foot pain (Morton’s Foot) to chronic pain and other problems throughout the body (Rothbarts Foot and PreClinical Clubfoot Deformity.
The following is an explanation of the structure, function, appearance, symptoms, prevalence and treatment of these four-foot structures:
Structure
Plantar Grade Foot
- Structurally stable. The calcaneus and talus bones have completed their ontogenetic torsional development. These bones do not maintain an abnormal torsion (twist).
Morton’s Foot (also called Morton’s Toe and Greek Foot)
- Discovered by Dudley Morton, is described as; a congenital short first metatarsal bone, hypermobile first metatarsal segment and posteriorly located sesamoid bones (See photos below).

Mortons Foot
Black arrow points to the congenitally short 1st metatarsal
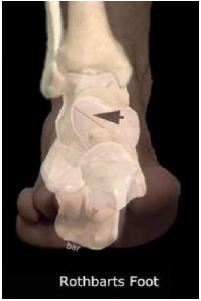
Rothbarts foot (originally termed the Primus Metatarsus Supinatus)
- Discovered by Professor/Dr Brian A. Rothbart in 1988, is an unstable, abnormal foot structure present at birth. It is the result of an incomplete torsional development of the talus, resulting in an elevated and inverted big toe and first metatarsal.
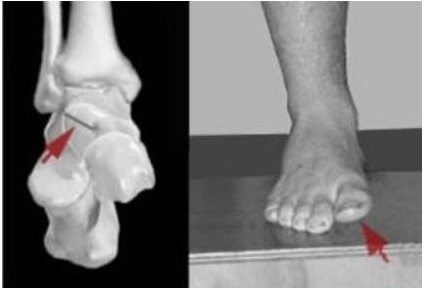
Red arrow (left photo) points to the incomplete torsional development of the talus.
Red arrow (right photo) shows the elevated and inverted big toe and first metatarsal.
Rothbarts Foot showing incomplete talus and inverted big toe
PreClinical Clubfoot Deformity
- Discovered by Professor/Dr Brian A. Rothbart in 2002. It has a more pronounced structural deformity compared to the Rothbarts Foot. Specifically; the Preclinical Clubfoot Deformity is the result of an incomplete torsional development of both the calcaneal (heel) and talar bones.
PreClinical Clubfoot Deformity
Function
Plantar Grade Foot
- Functionally stable. The first metatarsal head bears the majority of the body´s weight in preparation for pushing off the big toe as you walk. The bottom of the foot makes contact with the ground without abnormally pronating (twisting inward and downward).
Morton’s Foot
- The first metatarsal is shorter than the second metatarsal, the body's weight is automatically transferred to the longer second metatarsal head.
Rothbarts Foot
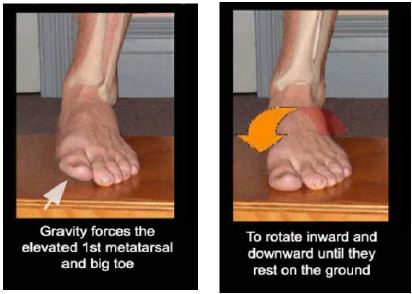
Gravity upon Rothbarts Foot
- The big toe and adjoining first metatarsal are both elevated and twisted inwards relative to the ground when the subtalar joint (rear foot) is placed in its anatomically neutral* (correct) position.
- As your body’s weight is shifted from your heel to the front of your foot (standing or walking), gravity forces your elevated big toe and adjoining first metatarsal to roll inward, forward and downward until they rest on the ground.
- (called foot twist or abnormal pronation).
PreClinical Clubfoot Deformity
- Produces more severe and prolonged foot twist (when you stand and walk) compared to a Rothbarts Foot;
- The result of the incomplete ontogenetic development of the calcaneus and talus is that when the rear foot is placed in its anatomically neutral* position, both the inside bottom surface of the heel bone and the big toe and its adjoining metatarsal are elevated and inverted relative to the ground;
- As the body’s weight lands on the heel, gravity forces the heel bone to twist inward and downward until the entire heel bone rests on the ground. This motion collapses the arch of the foot as the body’s weight is transferred to the front of the foot. Gravity then forces the elevated big toe and adjoining metatarsal to roll inward, forward and downward until they also rest on the ground;
Note – Because the Rothbarts Foot and PreClinical Clubfoot Deformity can functionally look very similar, the only way to determine which of the two structures you actually have, is by running specific computer and video analyses.
Appearance
Plantar Grade Foot
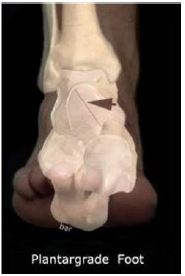
Plantargrade Foot
The black arrow points to the complete torsional development of the talus resulting in the big toe and adjoining metatarsal naturally resting on the ground.
- There is no elevation of the big toe. That is, when the foot is placed in its anatomical neutral position, the big toe and adjoining metatarsal rest on the ground. Walking, there is no visual foot twist as the weight of the body is transferred from the heel bone, across the midfoot to the forefoot.
.
Morton’s Foot

Mortons Foot Congenitally Short 1st Toe
White arrow points to the congenitally short 1st toe
- The big toe is more than 2mm shorter than the second toe (See Photo above).
Rothbarts Foot
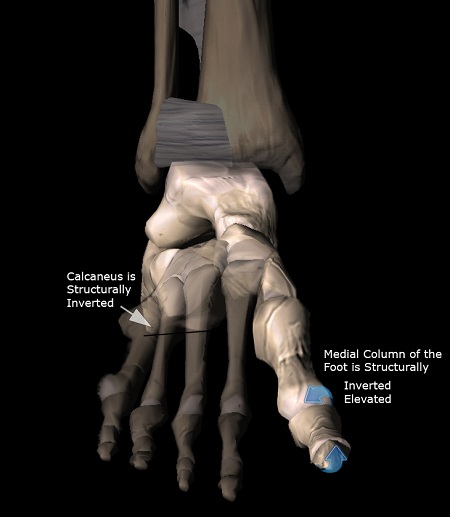
Rothbarts Foot Incomplete Torsional Development
The black arrow points to the incomplete torsional development of the talus resulting in an elevated and inverted big toe and metatarsal when the foot is placed into its' anatomically
neutral position
- It’s not easy to see a Rothbarts Foot by merely looking at your feet. The elevated and inwardly twisted big toe and first metatarsal, resulting from an incomplete torsional development of the talus, can only be seen when the rearfoot (subtalar joint) is placed in its anatomically neutral position.
The only way to 100% determine that you have a Rothbarts Foot is by looking at the bones inside your feet. A WBCT [weight-bearing computed tomography] of the talar head provides a definitive diagnosis. However, there are indicators that the Rothbarts Foot is present, such as;
- 8 or more positive responses from the Rothbarts Foot Questionnaire;
- The BioVector Measurement test and the Three Minute Screening for Rothbarts Foot, both of which I developed, quantify the presence of the elevated big toe and first metatarsal when your foot has been placed in its anatomical neutral position;
- Computerized gait analyses rule in (or out) whether you walk in a predefined way (consistent with the walking motion of a person with a Rothbarts Foot).
PreClinical Clubfoot Deformity
- It’s not easy to see the PreClinical Clubfoot Deformity by merely looking at your feet. The inwardly twisted and elevated calcaneus, first metatarsal and hallux (big toe) that characterizes the PreClinical Clubfoot Deformity can only be seen when the rearfoot (subtalar joint) is placed in its anatomically neutral position.
- The only way to 100% determine that you have a PreClinical Clubfoot Deformity is by looking at the bones inside your feet. A WBCT of the posterior aspect of the calcaneus and talar head provides a definitive diagnosis.
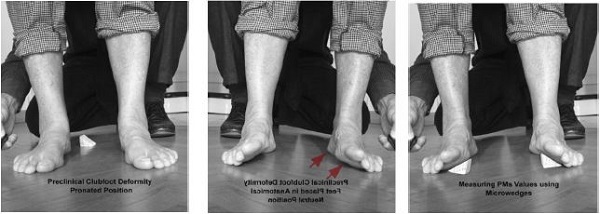
BioVector Measurement Test
BioVector Measurement Test - The Primus Metatarsus Supinatus (PMS) measurement quantifies the distance between the elevated first metatarsal and ground. Note the elevated and inverted position of the first metatarsal, adjoining big toe and calcaneus (See Redarrows) when the foot is placed into its' anatomical neutral position.
Indicators that the PreClinical Clubfoot Deformity is present:
- Your responses to the questions asked in the Rothbarts Foot Questionnaire and in my patient profile (during your Initial Phone Consultation).
- Computerized gait analyses rule in (or out) whether you walk in a predefined way (consistent with the walking motion of a person with a PreClinical Clubfoot Deformity).
- The BioVector Measurement test shows the presence of the elevated big toe, first metatarsal and calcaneus when your foot has been placed in its anatomical neutral position (See 3 photos above).
Because the Rothbarts Foot and PreClinical Clubfoot Deformity can visually look very similar, a differential diagnosis is obtained by running specific clinical, computer and/or video analyses.
Symptoms
Plantar Grade Foot
- If you have a plantar grade foot, you will have healthy feet, free from foot pain. You will also have good posture, and because of this, you’ll most likely never suffer with chronic muscle and joint pain or other health problems that are caused by bad posture.
Morton’s Foot
If you have a Morton’s Foot, you will have foot pain. This is because the second metatarsal head (due to its smaller size) is not meant to support the majority of the body's weight. The results can be:
- The body protects the (smaller and more fragile) second metatarsal head by building up callus tissue, which feels like a pebble imbedded in the skin and produces pain when you walk;
- The second metatarsal head may fracture because it’s not robust enough to take the body’s weight;
- The second metatarsal head could become inflamed.
Note – My research concurs with Dudley Morton's findings, in that the Morton’s Foot mainly produces painful symptoms in the feet. But recently, some internet sites (talking about the Morton's Foot) have cited Janet Travell's earlier work, which suggests that Morton's Foot is a common perpetuator of chronic musculoskeletal pan throughout the body.
It needs to be clarified; when I worked with Travell in her later years, she told me that what she thought was Morton's Foot was in fact, Rothbarts Foot. This is because; in a Morton’s Foot, the first metatarsal is shorter than the second metatarsal, and in a Rothbarts Foot, the first metatarsal is elevated and twisted inward (so it may appear shorter than the second metatarsal – when in actuality it is not).
Rothbarts Foot
- The Rothbarts Foot causes not only foot pain, but also bad posture. This bad posture leads to chronic muscle and joint pain, as well as other problems throughout the entire body.
PreClinical Clubfoot Deformity
- The PreClinical Clubfoot Deformity typically creates worse posture than the Rothbarts Foot. The result is severe, debilitating chronic muscle and joint pain, as well as a plethora of chronic problems throughout the body.
Prevalence
Plantar Grade Foot
- The plantar grade foot is relatively uncommon. About 10% of the world population is fortunate enough to have this foot structure.
Morton’s Foot
- The Morton’s Foot is a relatively uncommon foot structure. Although Morton's Foot is a disorder, many healthcare providers simply believe it to be a normal variant of foot shape, affecting 10-30% (depending on the author) of the population;
- My experience has shown that this foot structure occurs in approximately 10% of the world population (more common in some parts of the world than others).
Rothbarts Foot
- The Rothbarts Foot is a relatively common foot structure. According to my findings, based on 45 years of research and clinical experience, it affects approximately 35 – 40% of the world population.
PreClinical Clubfoot Deformity
- The PreClinical Clubfoot Deformity is a relatively common foot structure. According to my findings, it affects at least 30% of the world population.
Treatment
Plantar Grade Foot
- The plantar grade foot needs no treatment or therapy.
Morton’s Foot
- The Morton’s Foot is effectively treated by using an extension pad extending from the 1st metatarsal head, past the big toe.
Rothbarts Foot
- Prescribing proprioceptive insoles specifically designed to stabilize this foot structure.
PreClinical Clubfoot Deformity
- Prescribing proprioceptive insoles specifically designed to stabilize this foot structure.
Reference Note
*Anatomical neutral position - The subtalar joint is in its anatomical neutral position when its joint spaces from front to back and side to side are uniform and even. That is, there is no deviation or variance in the thickness of the joint space from side to side and front to back.
Comments:
-
No Article Comments available