Positive Health Online
Your Country

![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Human Kinetics Trail Guide to the Body]](/img/original/TopicbannerAvatar/4656.d9ccc329faa3d1500b4807b369feccef.jpg "Human Kinetics Trail Guide to the Body")
![[Image: Lotus Books]](/img/original/TopicbannerAvatar/953.adb373b0210368e0c9ce4d9a8a9f01aa.jpg "Lotus Books")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
Simplified Musculoskeletal Assessment System
by Dr Anthony Lombardi(more info)
listed in bodywork, originally published in issue 204 - March 2013
Manual medicine needs a standardized system for the assessment of musculoskeletal injuries to help ensure consistent quality in clinical outcomes.

The conventional assessment of these types of injuries has traditionally been performed in a vacuum. A doctor treating a patient with elbow pain typically performs elbow orthopaedic testing, while a patient with low-back pain undergoes an exam that focuses on straight-leg raise (SLR) and sacroiliac joint (SI) tests. Patients with non-traumatic knee pain undergo every knee orthopaedic test imaginable until the doctor draws his or her own conclusion. Conventional assessment approaches often lead to incorrect interpretations of the diagnostic imaging that has been ordered.[22, 25, 27] When injuries are assessed in a vacuum, there are often discrepancies among the different diagnoses. As a result, you order several different tests to zero in on the condition. You look for and expect answers in the imaging because the assessment wasn’t specific enough. Practitioners often use the results of imaging to bring clarity to their diagnosis, yet their interpretation of the imaging results can be inaccurate.[22]
As clinicians we are presented with injuries and different clinical presentations that challenge the way we assess our patients. MRI and ultrasound imaging are common diagnostic tools used by doctors and therapists in determining tissue injury. However, several landmark studies have shown that tissue tears revealed on such imaging are very common in patients who are completely asymptomatic.[22-27] Since there is a lack of a causal relationship between diagnostic imaging results[22,23] orthopaedic testing,[27] and symptoms,[24] we must look further into what is happening on a musculoskeletal level when patients are experiencing pain and dysfunction.
A New England Journal of Medicine study[22] revealed that in a MRI examination of the lumbar spine, many people without back pain have disk bulges or protrusions. Given the high prevalence of these findings and of back pain sufferers, the discovery of bulges or protrusions by MRI in people with low back pain may frequently be just coincidental. A study focusing on rotator cuff tears[23] determined that approximately 40 percent of asymptomatic patients over the age of 50 have full-thickness rotator cuff tears. In a research paper[24] it was reported that the high incidence of asymptomatic tears in the study group indicate rotator cuff tears can be regarded as a natural correlate of ageing and that bilateral tears are common. There is an over-reliance on single orthopaedic tests which is unreliable[27] in clinical environments when assessing musculoskeletal dysfunction, and there is a lack of research to support conventional orthopaedic testing.[25]
A Change in Thinking
Rather than using conventional testing, practitioners should look at restoring dysfunction in the musculoskeletal system by locating and restoring motor muscle inhibition. The three factors that that cause motor muscle inhibition are nociception, pain, and arthrogenous changes. Since motor inhibition due to one or more of these factors is a common theme in all musculoskeletal injury[3-15] it is vital to assess how motor muscle inhibition affects the biomechanics of the injured patient. These findings are more consistently present in the functional assessment of musculoskeletal injuries[28] while more conventional findings such as disc bulges, muscle tears, and orthopaedic testing results are findings which are less consistent in our clinical reasoning of musculoskeletal dysfunction.[22-27] More manual therapists are taking a more contemporary approach by focusing on motor muscle inhibition by creating a standardized assessment system[28,29] to help recognize motor inhibition in the musculoskeletal system and are able to use such therapies as myofasical release, joint manipulation and electro-acupuncture to restore dysfunction.[21,28]
One of the biggest mistakes practitioners make during musculoskeletal exams is that they initially assess or focus on the area of pain. Doing so narrows your clinical mind. Barring direct traumatic injury, the area of pain should be the last place assessed.
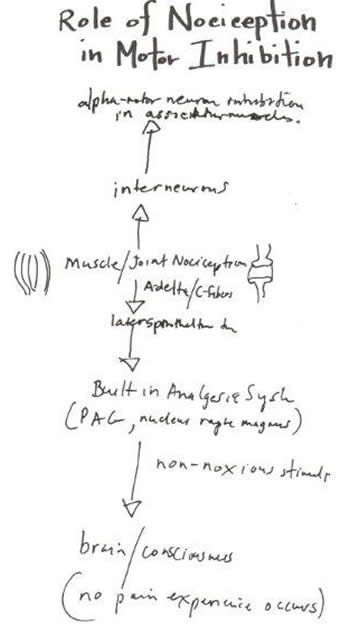
Role of Nociception in Motor Inhibition
Pain is a consequence - not the cause - of patients’ problems. Nociception can be stimulated from different areas[5,6] via a combination of:
- Local factors like myofascial or periosteal trigger points;
- Regional factors like neurometabolic segmental articular dysfunction;[1,2]
- Global factors like autonomic nervous system dysfunction.
Therefore, the assessment must be multi-dimensional in nature. The emergence of a new consensus is changing the way assessments are done. A study in the Journal of Athletic Training observed that the musculoskeletal system is made up of basic skeletal foundations: the scapular girdle and pelvic girdle, which become inhibited during injury or dysfunction.[14,31] The soft tissue and peripheral nerves connect to or interact with these skeletal girdles. Also, the kinetic chain of movement in the extremities begins in one or both of these skeletal girdles. Therefore, longstanding elbow pain cannot be present without some degree of shoulder girdle dysfunction and/or longstanding shoulder pain cannot be present without some degree of elbow or wrist dysfunction.
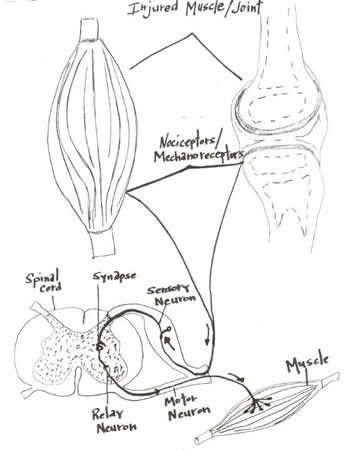
Injured Muscle Joint
Injuries related to soft tissue are likely not isolated to one area or one joint. A shoulder problem carries elbow and wrist dysfunction.[13] Conversely, low-back pain and sacroiliac pain is often associated with dysfunction of the tissues that support the pelvic girdle and stabilize the lumbar spine. A simplified musculoskeletal assessment system[30] is needed to assess global mechanical function of the body. This system would provide information in minutes - about the nature of the dysfunction, the adaptability of the tissues, and the origin of nociception. By doing this, treatment can be focused on correcting mechanical dysfunction, which in turn will address the chief complaint.
A New Simplified Assessment System
The contemporary simplified assessment[30] approach focuses on revealing and restoring musculoskeletal inhibition which can be completed in 2-3 minutes.
Step 1: Movement Analysis. Musculoskeletal assessment should never be performed without an analysis of gait and functional movements. Watching how the body interacts with gravity is necessary when dealing with these types of injuries;
Step 2: Palpatory exam. This allows you to find and appreciate areas of trophic change and areas of trophedema. These regions are products of neurogenic inflammation from the sensory axons, which can trigger plasma extravasations that lead to abnormal collagen scar tissue formation.[5,6]
These changes are present months - even years - prior to the patient experiencing pain, stiffness, etc.
Step 3: Skeletal foundation assessment. The largest component is the assessment of the skeletal foundations (shoulder girdle, pelvic girdle) and the local assessment of tissues along the kinetic chain of movement. The body is in a constant state of adaptation. You need to understand how the body works on both a mechanical and a neurometabolic cellular level. This way, you can learn to appreciate the nature of the dysfunction and how to correct the problem. Understand that no issue is one-dimensional. Neck pain has contributions from neck and shoulder dysfunction, while shoulder pain can be a product of neck and shoulder limitations with associated upper extremity adaptation.[6]
How Do You Restore Motor Muscle Dysfunction Once You Find It?
Acupuncture,[16,17] needle injections,[17,18] intramuscular stimulation,[17,19] joint manipulation,[20] and myofascial release[21] have been demonstrated to restore motor neuron function in many documented studies. The limitations, however, lie in the ways chiropractors and therapists perform assessments, which differ greatly from practitioner to practitioner. A motor adaptation is essentially a response to a failure somewhere in the musculoskeletal system. The sooner clinicians are able to process that information, the sooner the appropriate therapies can be applied to restore the system to health.
Here is an example of two case studies of simplified assessments using a specific assessment system.[30]
Case 1
25-year-old female presents with R ‘tennis elbow’ pain of 4 months' duration. She is a competitive squash player and has had to modify her stroke to compensate for the elbow pain. NSAIDs and ice give her temporary relief. The simplified assessment system[30] reveals on gait analysis that her right arm swings considerably less than her left and the right trapezius is elevated during her gait. The upper body scan reveals her cervical rotation (45 degrees on visual inspection) and lateral flexion is very limited to the right. Marked weakness occurs upon testing the supraspinatus in both positions and her serratus anterior is inhibited.
Typical Diagnosis:
R ‘tennis elbow’
Specific Direction Treating Practitioner Needs
R lateral elbow pain associated with limited R cervical spine rotation/ lateral flexion and weakness (inhibition) of the supraspinatus and serratus anterior muscles.
Treatment Executed
Electro-acupuncture to the motor points of the serratus anterior and supraspinatus muscles followed by myofascial release. Once inhibited, muscles are restored then focus on improving perfusion to the muscles of the cervical spine by using segmental acupuncture along the paraspinal muscles extending from T1-T6 to affect the inferior cervical sympathetic chain which has arterial control of blood flow to the head, neck , and upper extremities.
Case 2
65-year-old male with moderate degenerative osteoarthritis in his lumbar spine presents with L lateral knee pain. Patient presents with good overall health, blood work is unremarkable, and x-ray reveals mild osteoarthritis in his left knee. The simplified assessment system 30 reveals a mild antalgic limp [form of gait abnormality where the stance phase of gait is abnormally shortened relative to the swing phase] during gait analysis and very little pelvis rotation during gait. The lower body scan reveals that standing lumbar extension is limited due to mild pain and upon strength testing of his oblique/ transverse abdominus he cannot stabilize his lumbar spine during resisted L lumbar rotation. The abductors pelvic girdle (TFL, gluteus medius) are inhibited on the right during stability testing.
Typical Diagnosis
L knee osteoarthritis
Specific Direction Treating Practitioner Needs:
L lateral knee pain associated with weak abdominal stabilizers and weak L sided hip abductors.
Treatment Executed:
Due to a fear of needles, electro-acupuncture cannot be performed with this patient. Otherwise, the simplest approach would be to restore inhibition of the abductors by stimulating the motor points with electro-acupuncture. However, I am still able to restore motor inhibition through the manual myofascial release of the psoas, TFL, and gluteus medius muscles and by using a jade / guasha tool along the surface of those muscles and the surface of the neighbouring iio-tibial band. Also, mobilization of the talo-crural joint will also bring temporary restoration of the abductor muscles.[31]
In your busy practice we must maximize the time we have with each patient. by using a simplified assessment system based on peer- reviewed research; we can discover dysfunction in minutes so that we can begin helping our patients immediately. Conventional assessment fails because it doesn’t consider the kinetic mechanical adaptation of the musculoskeletal through motor inhibition and the peripheral nervous systems. The value of a focused assessment examination is worth exponentially more than any amount of treatment. It is priceless.
References
1. Devor DC, Singh AK, Lambert LC, DeLuca A, Frizzell RA, Bridges RJ. Bicarbonate and chloride secretion in Calu-3 human airway epithelial cells. J Gen Physiol 113(5):743-60. 1999.
2. Ljung BO, Alfredson H, Forsgren S. Neurokinin 1-receptors and sensory neuropeptides in tendon insertions at the medial and lateral epicondyles of the humerus. Studies on tennis elbow and medial epicondylalgia. J Orthop Res. 22(2):321-7. 2004.
3. Cote JN, Hoeger-Bement MK. Update on the relation between pain and movement: consequences for clinical practice. Clinical Journal of Pain. 26:754-762. 2010.
4. Portenoy RK, Thaler HT, Kornblith AB. Symptom prevalence, characteristics and distress in a cancer population. Qual Life Res 3:183–89. 1994.
5. Baluk P. Neurogenic inflammation in skin and airways. Investig Dermatol Symp Proc. 2(1):75-81. 1997.
6. Nijs J, Daenen L, Cras P, Struyf F, Roussel J, Oostendorp R. Nociception affects motor output: a review on sensory-motor interaction with focus on clinical implications. Clinical Journal of Pain. 28(2):175-181. 2012.
7. Zimmermann M. Pathophysiological mechanisms of fibromyalgia. Clinical Journal of Pain 1991: Suppl 1:S8-15.
8. Lund JP, Donga R, Widmer CG, Stohler CS. The pain-adaptation model: a discussion of the relationship between chronic musculoskeletal pain and motor activity. Can J Physiol Pharmacol. 69(5):683–694. 1991.
9. Svensson P, Arendt-Nielsen L, Houe L. Sensory-motor interactions of human experimental unilateral jaw muscle pain: a quantitative analysis. Pain. 64(2):241-9. 1996.
10.Stokes M, Young A. The contribution of reflex inhibition to arthrogenous muscle weakness. Clin Sci.67(1):7–14. 1984.
11. Hurley MV, Newham DJ. The influence of arthrogenous muscle inhibition on quadriceps rehabilitation of patients with early unilateral osteoarthritic knees. British Journal Rheumatology. 32:127-131. 1993.
12. Hurley M, Scott DL, Rees J. Sensorimotor changes and functional performance in patients with knee osteoarthritis. Ann Rheum Dis. 56:641- 8. 1997.
13. Horre, Osnabruck The Influence of Joint Dysfunction on Muscle Function (dissertation). 2006.
14. Sedora JD. Arthrogenic muscle response of the quadriceps and hamstrings with chronic ankle instability. Journal of Athletic Training. 42(3):355-360. 2005.
15. Ingersoll CD, Palmieri RM, Hopkins JT. A joint dilemma. Rehab Management 16(1):38-42 . 2003.
16. Xiao-Hong C. Optimal conditions for eliciting maximal electroacupuncture analgesia with dense-and-disperse mode stimulation. American Journal of Acupuncture 22(1):47-53. 2002.
17. Lewit K. The Needle Effect Of Myofascial Pain. Pain 6(1):83-90. 1979.
18. Staud R. Are tender point injections beneficial: the role of tonic nociception in fibromyalgia. Curr Pharm Des.12(1):23-7. 2006.
19. Gunn CC, Milbrandt WE, Little AS, Mason KE. Dry needling of muscle motor points for chronic low-back pain: a randomized clinical trial with long-term follow-up. Spine 5: 279–91. 1980.
20. Dishman D, Burke JM, Cunningham B. Comparison of tibial nerve H-reflex excitability after cervical and lumbar spine manipulation. Journal of Manipulative and Physiological Therapeutics. 25(5):318–325. 2002.
21. Schleip R. Fascial plasticity – a new neurobiological explanation. Journal of Bodywork and Movement Therapies. 7(1):11-19 and 7(2):104-116. 2003.
22. Jensen M. Brant-Zawadzki N. Obuchowski N. Modic M. Malkasian D. Ross J. Magnetic Resonance Imaging of the Lumbar Spine in People without Back Pain. New England Journal Of Medicine. 331:69-73. 1994.
23. Worland R. Lee D. Orozco C. SozaRex F. Keenan J. Correlation of age, acromial morphology, and rotator cuff tear pathology diagnosed by ultrasound in asymptomatic patients. Journal of Southern Orthopedic Association. 12(1): 23-26. 2003.
24. Oschman Z. van Rensburg C. Maritz N. Boraine H.Owen R. Ultrasound study of the asymptomatic shoulder in patients with a confirmed rotator cuff tear in the opposite shoulder. SAJSM. 19(1): 121-128. 2007.
25. Cadogan A. Laslett M. Hing, W. McNair P. Williams M. Interexaminer reliability of orthopaedic special tests used in the assessment of shoulder pain. Manual Therapy. 16(2): 131-135. 2011.
26. Simpson R. Gemmell H. Accuracy of spinal orthopaedic tests: a systematic review. Chiropr Osteopat. 14(31): 26-29. 2006.
27. Contant L. The Efficacy Of Lumbar Spine Orthopedic Testing - A Literature Review. www.logan.edu/mm/files/LRC/Senior-Research/2003-Aug-07.pdf 1-18. 2003.
28. Lomond J. Case Study Assessment And Treatment Approach Of A Therapist. In: Contemporary Integrative Dry Needling, Vol. 1, 1st Ed., Pgs 158-170. New York: Elsevier. 2012.
29. Lombardi A. A New Angle On Assessment. Chiropractic Economics. 58(15):25. 2012.
30. Lombardi A. EXSTORE Assessment System: Chiropractors & Manual Therapists Edition, AJL Publishing Company, Hamilton, Ontario, Canada.
31. Gribble PA, Hertel J, Denegar C. Chronic ankle instability is associated with strength deficits in proximal lower extremity muscle groups [abstract]. J Athl Train. 40:S-28 (suppl). 2005.
About the Author
Dr Anthony Lombardi DC is the owner/founder of Hamilton Back Clinic, a multidisciplinary practice in Hamilton, Ontario, Canada. He is a consultant to athletes in the NFL, NCAA, CFL, and NHL. He has written and published a book/dvd work: EXSTORE Musculoskeletal Assessment System. To reach Dr. Lombardi, visit www.exstore.ca
Comments:
-
Edward Jarvis said..
This makes perfect sense to me, I know it is right. We have the one eye, in the land of the blind. Explaining this to patients is needed, so they understand that Exstore and motor point acupuncture is "the way". Thank you Anthony.