Positive Health Online
Your Country

![[Image: https://www.water-for-health.co.uk/]](/img/original/BannerAvatar/4046.12831f50177f8848ee87b8e94411d6b3.jpg "https://www.water-for-health.co.uk/")
![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: https://peacegifts.shop/]](/img/original/BannerAvatar/3906.e1d1ebc07ce7530bbb3d6cf426966b6f.jpg "https://peacegifts.shop/")
![[Image: http://www.balens.co.uk]](/img/original/BannerAvatar/2148.50367fa908013fae0a7f1a171543ef92.jpg "http://www.balens.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Lotus Publishing]](/img/original/TopicbannerAvatar/953.adb373b0210368e0c9ce4d9a8a9f01aa.jpg "Lotus Publishing")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
Gleno-Humeral Joint and Upper Extremity Examination: Evaluation & Treatment
listed in osteopathy, originally published in issue 218 - November 2014
Gleno-Humeral Joint / Shoulder Complex
The main function of the gleno-humeral joint is to place the hand where it is needed, but to achieve this you have flexibility at the expense of stability. The shoulder is not just one joint but 4 inter reacting joints.
I. The gleno-humeral joint (the true shoulder joint)
II. Acromio-clavicular joint
III. Sterno-clavicular joint
IV. Scapulo-thoracic joint
Muscles of the Shoulder Joint Complex
| Flexion | Pec major, coracobrachialis, anterior fibres of deltoid. |
| Extension | Teres major, lat dorsi, posterior fibres of deltoid. |
| Abduction | Supraspinatus (initiates abd) and assists mid deltoid. |
| Adduction | Pec major and latisimus dorsi. |
| Internal Rotation | Teres major, subscapularis, pec major, anterior deltoid. |
| External Rotation | Infraspinatus, teres minor and posterior deltoid. |
| Retraction | Rhomboid major and minor. |
| Protraction | Serratus anterior, pecs |
It is important to fully understand the location and function of the muscle groups that stabilize and achieve the movements of the shoulder complex. So as to work out the numerous dysfunctional conditions that can manifest in the shoulder complex.
The strong tendons around the joint achieve certain stability. However they do not prevent inferior dislocation, a common shoulder problem. Due to the shallow glenoid fossa, weak coracohumeral ligament, laxity of the joint capsule and the horizontal arrangement of the rotator cuff which comprises supraspinatus, infraspinatus, teres minor & subscapularis.
The long head of biceps arises from the superior glenoid fossa / labrum and has to penetrate the joint capsule before entering the intertubercular groove and its sheath of synovial membrane. Due to this passage through the joint capsule inflammation to long head of biceps can easily spread to the capsule resulting in capsulitis that could become adhesive. Longhead of triceps arises from the inferior glenoid fossa / labrum and also penetrates the joint capsule, which could lead to capsular inflammation but is quite rare.
Gleno-humeral abduction consists of two phases;
- 0 → 90° supraspinatus & deltoid.
To go further requires scapular rotation achieved by; - 90 → 180° trapezius/ lev scapulae whilst stabilized by serratus anterior.
Pain noted between 80→120° is known as painful arc and is usually an indication of subacromial bursitis/supraspinatus tendonitis.
It should also be noted that during the middle phase of abduction there is a mild contraction of triceps via its long head to pull down the head of the humerus thereby preventing it coming into excess contact with the sub-acromial articulating surface. However over a period of time if triceps becomes weak (‘bingo-wing syndrome’) or patient over trains / develops biceps the humeral head will make excess contact with the sub-acromial articular surface resulting in inflammation and early arthritic change. This can be assisted by giving straightforward exercises to improve the tone of triceps.
Flexion going forward is achieved by anterior deltoid, coracobrachialis and pec major up to 60° before the scapula and shoulder girdle have to move. This is achieved by serratus ant and upper trapezius tipping the scapula, elevating the acromion resulting in axial rotation at the acromioclavicular (A/C) and sternoclavicular (S/C) joints.
Internal rotation is achieved by Teres major, subscapularis, pec major, anterior deltoid.
External rotation is achieved by infraspinatus, teres minor and posterior deltoid. Clinically they are easily strained leading to fibrosis and shortening thereby limiting ‘internal’ rotation. For extreme external rotation to take place requires adduction of the scapula by rhomboids and lower trapezius, whereby the acromion gaps from the clavicle. Re-enforced external rotation by the operator can thus be used to test the ligaments of the A/C jt.
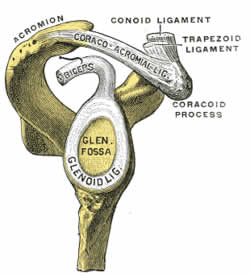
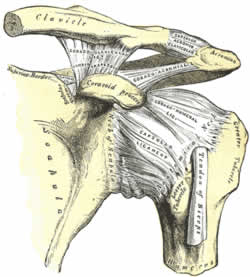
Ligaments
Gleno-humeral jt ligaments re-enforce the thin lax joint capsule.
I. Coracohumeral ligament, coracoid process to the greater tubercle, re-enforces the superior aspect of the jt capsule & checks external rotation.
II. Transverse humeral ligament attaches across the greater and lesser tubercles and holds the long head of biceps in the bicipital groove.
III. Acromioclavicular ligament is intrinsically weak supporting the superior aspect of the jt capsule.
IV. Coracoclavicular ligaments also support the A/C joint. These include the conoid and trapezoid ligaments which check superior movements of the clavicle on the acromion.
V. Conoid ligament, coracoid process to clavicle.
VI. Trapezoid ligament coracoid process to clavicle (distal)

Shoulder Joint Complex Evaluation.
The A/C joint is comparatively inflexible and weak given the constant stress and strain placed on the area through work, sports etc. It is therefore easily dislocated from a direct force from above resulting in sprain/tearing of the A/C ligament. Also fall on out stretched hand (FOSH) usually results in complete tearing of A/C and coracoclavicular ligaments with resultant dislocation of the joint. In severe trauma both sterno clavicular and costo clavicular ligaments also rupture (RTA).
Of the rotator cuff muscles the most commonly injured is supraspinatus. Poor blood supply/ nutrition to the area may not meet the demands of the tissues, resulting in an inflammatory response causing tendonitis, which if left to become chronic the body reacts by laying down scar tissue and even calcium deposits. This fundamentally weakens the tendon and can lead to complete rupture as loss of initiation of abduction.

Test using the ‘empty can test’ arm abducted to 90° with thumb down, ask pt to resist your downward pressure® pain / weakness indicates supraspinatus tendonitis / tear.
Primary bursitis is rare and tends to be more secondary as a progression from unchecked tendonitis, usually supraspinatus. Chronic swelling & fibrosis of the tendon compresses the bursae under the sub coraco-acromial arch resulting in its swelling & inflammation. This produces the classic painful arc (80-120°) during abduction of the GH joint.
Adhesive capsulitis the exact cause of which still remains unknown, is generally accepted to be a progression of the tendono-bursitis phenomena that initiates inflammation and eventual adhesion of the GH capsule usually the slack postero-inferior fold. Also continued joint immobility can lead to capsular tightening and eventual fibrosis. Along with degenerative joint disease, rheumatoid arthritis and reflex sympathetic dystrophy. High incidence in diabetics.
Long head biceps tendonitis usually brought on by rpt strain / overuse / sport.
Winged scapula, weak serratus ant due to compression / avulsion long thoracic nerve C5, 6, 7.
The shoulder area is also a site of referred pain from:
- Cervical spine facets & nerve roots;
- Heart via left phrenic nerve;
- Liver & gall bladder via right phrenic n;
- Diaphragm;
- Breast.
Remember that most of the muscles responsible for shoulder movement receive innervation from C5 / 6 hence the importance of evaluating the neck as well.
To evaluate the movements of the GH jt, A/C and S/C go to 7 stages of Spencer etc.
- Observation;
- Active;
- Passive;
- Active resisted muscle testing;
- Special tests.
Treatment
Success in the treatment for dysfunction of the shoulder complex depends upon the accurate determination of the underlying cause. This may present a formidable challenge, as the true cause may lie somewhat distant to the site of pain.eg; dysfunctional movement of the humeral head in the glenoid may be caused by restrictions of scapular rotation, leading to capsulitis / bursitis. Thus underlying secondary or predisposing factors will need to be removed first before correction of the primary condition can be accomplished. Also the pain of acute capsulitis of the G/H may be so extreme as to demand palliative procedures initially i.e. ice, NSAIDs, dry needling, rest before manipulation for correction of the basic cause can be tolerated.
Comments:
-
No Article Comments available