Positive Health Online
Your Country

![[Image: https://www.water-for-health.co.uk/]](/img/original/BannerAvatar/4046.12831f50177f8848ee87b8e94411d6b3.jpg "https://www.water-for-health.co.uk/")
![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: https://peacegifts.shop/]](/img/original/BannerAvatar/3906.e1d1ebc07ce7530bbb3d6cf426966b6f.jpg "https://peacegifts.shop/")
![[Image: http://www.balens.co.uk]](/img/original/BannerAvatar/2148.50367fa908013fae0a7f1a171543ef92.jpg "http://www.balens.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: Lotus Publishing]](/img/original/TopicbannerAvatar/953.adb373b0210368e0c9ce4d9a8a9f01aa.jpg "Lotus Publishing")
![[Image: Turning Point]](/img/original/TopicbannerAvatar/981.28945ea95f14bc185effb4ae6d8a75ab.jpg "Turning Point")
Cranial Osteopathy
listed in osteopathy, originally published in issue 18 - March 1997
To understand cranial osteopathy it is necessary to understand osteopathy itself. As with visceral osteopathy, the term refers to an aspect of osteopathy, not to a separate modality.

Saggital Section: Head & Neck
Given that osteopathy is about to be confirmed as a statutorily self-regulated profession in the United Kingdom it is opportune to refer back to its origins in the last half of the 19th century. Andrew Taylor Still, born in Virginia in 1828, engineer and then army surgeon during the American Civil War, became dispirited with the medical shortcomings of his day with its indiscriminate drugging and brutal surgery.[1] Spurred on, no doubt, by the deaths of his three children from 'spinal meningitis' he felt impelled to find more compassionate ways of dealing with medical problems. Osteopathy was the result

Sphenoid and occiput
In his book written in old age [2] at the turn of the century, Still describes osteopathy as "a scientific knowledge of anatomy and physiology in the hands of a person of intelligence and skill who can apply that knowledge to the use of people who are sick or wounded by strains, shocks, falls or mechanical derangement or injury of any kind to the body." Such a practitioner sees the potential for disease in the slightest anatomical deviation. A successful osteopath is or should be a "person of individuality with a mechanical eye behind all motions or efforts to readjust any part of the body to its original normality." Well-directed skill is essential rather than unguided force in giving relief.
Still goes on to describe the role in health and disease of essential tissue such as nerves, blood and lymph vessels, cerebrospinal fluid (CSF, he proclaims, is the highest known element in the human body – "a great river of life that must be tapped and the withering field irrigated at once or the harvest of health is forever lost'), fascia, the brain and spinal cord, the viscera (body organs] and the other fluids of the body. On page 46 he gives some cautionary advice: "Many of your patients are well six months before they are discharged. They continue treatments because they are weak and they are weak because you keep them so by irritating the spinal cord."
"Throw off your goggles," says Still, "and receive the rays of sunlight which forever stand in the bosom of Reason."

Sutural bevels to guide movement of bones
In appropriate context, throwing off the goggles seemed to reveal fertile ground for innovation. Chief amongst Still's disciples was William Garner Sutherland [3] who, 60 years ago, set out to demonstrate that, contrary to current belief, motion was possible and indeed existed in the sutures of the skull. He showed that there was at the same time a persistent involuntary movement of the tissues and organs such as the brain and spinal cord, the sacrum between the ilia [pelvic bones] and the trunk and limbs. He termed the whole process the Primary Respiratory Mechanism (PRM) – primary because he rated its significance to the onset of and departure from life above that of the heart or lungs.
The rate of movement of the PRM he called the cranial rhythmic impulse (CRI), a rhythm distinct from that of the other two. The CRI and the palpable movements of the body and of the CSF became of diagnostic and therapeutic importance in the total osteopathic approach to an individual. Sutherland's teachings were effectively presented by Harold Magoun in the first ever textbook for practitioners, [4] since when there have been numerous others. Among the most research-based are those of M.B. De Jarnette [5] and John Upledger. [6]
Why, then, the emphasis on cranial osteopathy as if it might supersede osteopathy, as if an arm and a leg (to be exact a head and a sacrum) were to become the body itself? Part of the trend is justified. Because of Sutherland and others some of the teachings of Still have been elaborated upon, made more of. To quote from Kimberly [7] "without the teachings of Sutherland at least one third of the autonomic system and two thirds of the central nervous system are being neglected in the consideration of the patient as an osteopathic whole." Made more of is the key phrase. Cranial osteopathy is not and should not be thought of as an exclusive, specialised programme of health care. Even less should there be a temptation to consider cranial osteopathy as a cure-all, however effective it is in many instances.
Figure 3 (above) The hazards of being a nerve
Fig 1 (above) Phenomena od the Primary Respiratory Mechanism
Sutherland's researches [8] are at the root of a variety of training programmes such as Sacro-Occipital Technic, Craniosacral Therapy, Craniopathy and Sutherland Osteopathy with its newly-titled concept of the Involuntary Mechanism. Students include masseurs, reflexologists, aromatherapists, kinesiologists and acupuncturists as well as osteopaths and chiropractors. From the orthodox professions come podiatrists, physiotherapists, dentists, midwives, medical doctors and nurses. In truth, there is no health care professional who would not benefit from some instruction in the cranial concept – it appears no longer to be the preserve of the osteopath. The last sentence reflects a much debated issue at present, something for the correspondence pages of this journal perhaps.
Individuals proceed through life by unveiling aspects of themselves as they mature. I doubt that they end up with characteristics additional to those with which they were born. In the same way, osteopathy as conceived by Still yields up facets of its inner truths with every new worker in the field. Sutherland was osteopathy's facet developer of inspired and painstaking quality. His product deserves the title cranial osteopathy. On a parallel course ran the lifetime of research that osteopath M.B. De Jarnette [9] developed for the chiropractic profession.
Every function depends upon an impulse generated in some part of the brain. If no impulse is generated the spinal cord has nothing to carry to any destination in the body. Whatever is best in therapeutics whether "cranial", surgical, medical or complementary is only as efficient as the cranium and its contents. The brain makes recovery possible. The message has to be developed before it can be delivered. The brain creates the message, the spinal cord delivers it and the pelvis (including the sacrum) must be in balance before any component can function efficiently.
Cranial osteopathy is not aggressive. It does not try to move the immovable. It is a gentle process of letting the respiratory system move the membranes of the internal cranial vault. Eight cranial and fourteen facial bones must articulate with each other so that all work together in harmony. Sutures (where cranial bones join each other) tie the cranial vault together and are lined by the tension membranes. Left and right membranes must be equal or at least they must synchronise with each other. All structures must be supplied with blood. Drainage systems must be kept open and draining. Lymph vessels must carry the products of metabolism unhindered from abdomen and chest to the heart. Mandibular articulation (the TMJ: temperomandibular joint) must be aligned for chewing food. The brain is the controller and with the hormonal system the coordinator of all such activities.
"Much energy," says De Jarnette, "is wasted by manipulators trying to make a vertebra replace the human brain." This is partly a reference to the limited approach of those osteopaths who do not include in their analyses the influence as well as the vulnerability of the cranial nerves within the skull. Cranial and sacral nerves are primarily parasympathetic autonomic controllers of all the senses, the movements of vital organs and the secretions of glands both endocrine and exocrine. There is more, therefore, to restoration of function than the adjustment of vertebrae, unless it is considered that the sphenoid bone which lies in the middle of the head is the uppermost vertebra of all.
The sphenoid is a shapely bone, not unlike a huge butterfly or moth and it articulates with the occiput at what is known as the sphenobasilar symphysis (sbs). Almost every bone in the head has a sutural junction with the sphenoid confirming the key role that the sphenoid plays in the integrity of the cranium. A blow anywhere on the head or face, a wisdom tooth pulled inexpertly, an unequal bite are examples of the ways in which the cranial bones and therefore their attached membranes can be distorted. Distortion can result in interference with any of the cranial nerves in the head and because of the fascial connection between occiput and sacrum there can be disturbances in the influence of sacral nerves as well.
The problem can be induced in the reverse direction almost as easily. A fall on the coccyx or a pelvic distortion because of a difference in leg lengths can malposition the sacrum within the iliac bones which in turn could offset the occiput and there onwards the sphenoid, the temporal or the parietal bones. If uncorrected, other cranial bones such as the frontal, zygomatic or maxillary can be affected. In time, cranial nerves can be disturbed as they pass through foramina (holes) in some of the bones and drainage from venous sinuses, such as that running along the inner surface of the parietal sagittal suture, can be impaired.
90+% of all blood from the head is drained through vessels that pass through the jugular foramen, a space between the temporal and occipital bones. Through the same foramen pass three cranial nerves, the Glossopharyngeal (IX), the Vagus (X) and the Spinal Accessory (XI). It is the Vagus that controls the sensations, activities and proprioception of many of the body's organs affecting breathing, circulation and digestion, while the other two influence such factors as taste, the ability to swallow, and the power to shrug the shoulders. Any of those functions can be affected, grossly or subtly, if the foramen is so disturbed by trauma or disease that the nerves and blood vessels that pass through it are compromised (see figure 3).
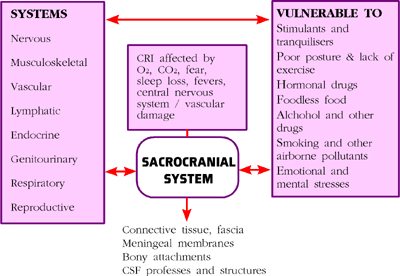
Fig 2 (above) Interactivity and Interdependance of the systems of the body and some threats to their functioning ability
Cranial osteopathy, then, is a structure-based system of medicine that calls into account all aspects of living, both causative and consequential. The primary respiratory mechanism is initiated at birth when the emergent baby becomes independent of mother's umbilical nourishment. It starts with an intake of breath followed by an out breath that is the listened-for first cry of the baby. The PRM ends its activities with a final breath out, hopefully a good number of years later.
None of the five components of the PRM shown in fig 1 exists on its own. It is the package as a whole that the sensitive practitioner is obliged to tune into. Figures 2 and 4 suggest that reasons for distress can stem from any system of the body, each in turn subject to external factors such as poor nutrition, polluted air, mento-emotional stresses and other influences that call for attention concurrently with hands-on treatment.
Fig 4 (above) Possible Causes and Effects of Disturbances of the Primary Respiratory Mechanism
Because of the extensive influence of the brain and nervous system, the circulation of the blood and the fluctuation of the cerebrospinal fluid on the musculoskeletal system and on all the organ systems of the body, it is not presumptuous to say that the osteopath, craniosacrally experienced, has resources to look into and sometimes help any patient.
Here follow some examples:
a brain damaged child of 18 months suffering 100 convulsions a day: attention to her eating habits and two cranially oriented treatments stopped her fitting entirely; treatment over subsequent years played a part in helping her to develop her personality and available faculties;
a man who, after dental treatment, had been unable to open his mouth more than half a centimetre for two days: one gentle palpation and encouragement to "locked" cranial bones including the sphenoid and temporals released his jaw;
varied patterns of headache relieved by releasing the frontal bone from the rest of the face or by lifting the parietal bones away from the temporals;
symptoms in parts of the body apparently unrelated to cranium or sacrum are analysed and dealt with by studying the fascial connections that may have become disturbed by, for example, an age-old fall or surgical operation.
To conclude, Cranial Osteopathy is an honourable but colloquial name to give to an inseparable component of health-promotion that encourages appropriate nourishment, structural integrity and psychological harmony of the individual being cared for. For those interested in pursuing the subject read Sutherland himself to start with.[10]
References
1 TRIANCE, Edward. Osteopathy, Thorsons, 1986.
2 STILL, Andrew Taylor. The Philosophy and Mechanical Principles of Osteopathy, Hudson Kimberly Publ, 1902 USA.
3 SUTHERLAND, William Garner. The Cranial Bowl, 1939.
4 MAGOUN, Harold I. Osteopathy in the Cranial Field, 3rd Ed 1976.
5 DE JARNETTE, Major Bertrand. Cranial Technique, Nebraska, 1979-1980.
6 UPLEDGER, John E. & VREDEVOOGD, Jon D. Craniosacral Therapy, Chicago, 1983 + others.
7 KIMBERLY, Paul E. Cranial osteopathy and its application. Lecture Des Moines Still College of Osteopathy and Surgery, October 23 1948.
8 GOODMAN, J. Chairman's Letter, Cranial Osteopathic Association Newsletter, Summer 1996.
9 DE JARNETTE, M.B. Lecture notes and personal communication on SOT
10 SUTHERLAND, Adah S. and WALES. Anne L. Collected writings of William Gamer Sutherland 1914-1954, The Sutherland Cranial Teaching Foundation USA, 1967.
Comments:
-
No Article Comments available