Positive Health Online
Your Country

![[Image: https://www.water-for-health.co.uk/]](/img/original/BannerAvatar/4046.12831f50177f8848ee87b8e94411d6b3.jpg "https://www.water-for-health.co.uk/")
![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: https://peacegifts.shop/]](/img/original/BannerAvatar/3906.e1d1ebc07ce7530bbb3d6cf426966b6f.jpg "https://peacegifts.shop/")
![[Image: http://www.balens.co.uk]](/img/original/BannerAvatar/2148.50367fa908013fae0a7f1a171543ef92.jpg "http://www.balens.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: ICAN International Clinical Aromatherapy Network]](/img/original/TopicbannerAvatar/4442.566a83a07de79de73b9c738f7fb6458a.jpg "ICAN International Clinical Aromatherapy Network")
![[Image: ISNS International Science and Nutrition]](/img/original/TopicbannerAvatar/4310.3fe1bd582f0b1b36c39fca00e3464581.jpg "ISNS International Science and Nutrition")
![[Image: SG Cancer Book]](/img/original/TopicbannerAvatar/960.4f24bbd158abe4427cc06911969143e5.jpg "SG Cancer Book")
Bone Building Nutrition - Calcium Not the Only Key
by Mark James Tallon(more info)
listed in nutrition, originally published in issue 92 - September 2003
Healthier Bones but at What Cost?
It is astounding that after all these years of education about the degenerative bone condition 'osteoporosis' in the UK, it is responsible for a fracture every 3 minutes.[1] Medical aid for the condition will cost the NHS 1.7 billion per annum, which levels out at 5 million each day.[1]
So why is this? With large ad campaigns aimed at building strong bones through optimum calcium (Ca) intake as the best defence against developing osteoporosis, why are the incidents of fracture so high?
Leading researchers in the field, like Dr Marcus Laux, a licensed naturopathic physician believe the answer may be in the application of calcium intake as the 'be all and end all' of osteoporotic prevention.
In the first comprehensive UK guide to bone health, this article gives you the facts and fallacies about calcium supplementation, traditional medicine and new clinically validated dietary solutions to healthier bones.
Bone Build-up and Breakdown
Every day of our lives our skeletal system, in one way or another, undergoes physiological and environmental stress and, as such, is remodelled. Our skeletal bone structure is made of a thick outer shell and a stronger inner mesh filled with collagen (protein), calcium salts and other minerals. Bones are truly amazing structures that mend and rebuild themselves by the actions of two cells types – osteoblasts that form bone and osteoclasts that resorb (destroy) bone. This continual process of breakdown and renewal is also known as bone turnover.
When the activity of the bone destroying osteoclastic cells outpaces that of bone-forming osteoblasts, the result can only be 'bone loss' and an increased risk of developing osteoporosis.
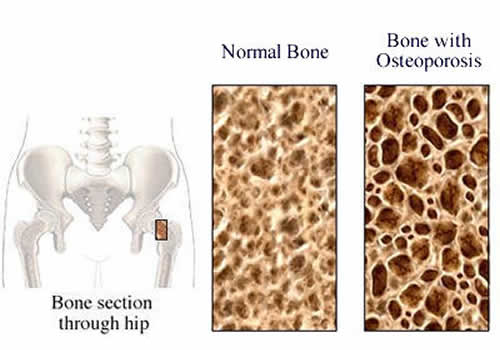
Osteoporosis – literally meaning 'porous bones' – is a condition that breaks down the skeleton making bones more fragile, resulting in an increased incidence of spontaneous fractures, especially in the vertebrae and hip. Bone loss from the osteoporotic condition can result in a healthy population for a variety of reasons, including insufficient dietary intake, pollutants, toxins, menopause, lack of physical activity and heredity. So what can be done to treat or regress the onset of bone disease?
Traditional Approaches to Bone Health
Traditional western medicine has had some success in the treatment of diseases and dietary deficiencies leading to bone loss. There are four main approaches that are used at present to help in the prevention of bone loss and increase bone mineral density (BMD).
BMD is often used as a marker of bone strength and health[2] and is the measurement of calcium in regions of the bone. Although it has an 85% prediction rate of detecting osteoporosis, it is far from fallible and should be backed up with urine analysis of collagen and deoxypyridinoline. Below is a brief on each, with some of the pros and cons associated with traditional medicinal treatments and their use.
Bisphosphates
In order of effectiveness, biophosphate therapy is the most successful treatment option with a decrease in vertebral fractures of about 30-49%.[3]
Calcitonin
Calcitonin nasal spray is not quite as effective as biphosphate but still has the ability to significantly increase BMD.[4] Nasal spray is a good option for late menopausal patients who cannot tolerate the gastrointestinal effects of biphosphates. Some clinicians consider it an initial option for the treatment of vertebral compression fractures in view of its reported analgesic effects.
Anitioestrogens
There is a class of pharmacopoeia know as selective oestrogen receptor modulators (SERMs) which you may have heard of as 'anitioestrogens'. The most commercially known name is probably Tamoxifen, which has the ability to bind oestrogen receptors.
Although it is not primarily prescribed for conditions such as osteoporosis, it definitely has skeletal effects by reducing bone turnover and thereby decreasing bone resorption.[5]
Raloxifen is also a SERM that reduces bone turnover to a similar degree as oestrogen and functions as an antiresorptive drug inhibiting osteoclastic activity. Although Raloxifene is very effective in reducing the risk of vertebral fracture, it was not as effective in reducing the risk of wrist, hip, or all nonvertebral fractures during two research trials.[6,7] On the down side, Raloxifene is associated with the risk of venous thrombolism to the same degree as oestrogen and, in addition, causes increased hot flushes.[8]
Hormone Replacement Therapy (HRT)
Hormone replacement therapy (HRT), as most of us know and many predicted, is in a state of confusion at present. Recent studies[9,10] reveal that it may not have the cardioprotective effect once associated with its use. Now multiple studies have, in fact, linked HRT use to incidences of increased breast cancer.[11] Over the past 5 years, these detrimental influences of HRT are gaining ever more scientific credibility. Women are now seeking alternatives to this approach to better bone health and, for these reasons, any impact on bone health through the use of HRT may be at a cost.
Natural Nutritional Therapies and Diet
Since bones are living tissues, bone cells need similar kinds of nutrients as other cells in our body. Over the past 20 years, substantial effort has been made toward increasing our understanding of the effect nutrition and dietary supplementation can have on bone loss with ageing (see Table 1). A new wealth of knowledge is now available. Thanks to the many milk-moustache ads of old, public education campaigns and the myriad of calcium fortified foods, the message seems to be clear – 'calcium saves bones for life'. However, as indicated earlier, there is much more to the nutrient story than calcium alone.
| Table 1:These are suggested recommendations based on the current scientific literature for adults. However before enrolling on any supplement plan you should first consult with a fully qualified physician or nutritional practitioner. | ||
| Food Substance | RDA(mg) | Therapeutic Dose(mg) |
| Calcium | 1000 – 1200 | 1000 – 0000 |
| Ipriflavone | N/A 200mg | 3x A day |
| Vitamin D | 5 – 15 mcg | 20mcg |
| Vitamin K | 55 – 70 mcg | 90-100mcg |
| Vitamin A | 1000mcg | 1000mcg |
| Vitamin C | 60 | 500 |
| Vitamin B12 | 6mcg | 6-10mcg |
| Magnesium | 310 | 600 |
| Zinc | 12 | 30 |
| Boron | No RDA available | 2- |
A number of vitamins, minerals and botanicals have emerged as key players in the bone-building story, and scientists are still working for a better understanding of their roles. Here is what we know so far…
Calcium – Fact versus Fiction!
Recent work has started to distinguish between osteomalacia (lack of dietary calcium) and osteoporosis (both a lack of calcium and other minerals), and as such this work is leading to a very different view of dietary and supplement food recommendations. Contrary to what the dairy industry tells us, milk consumption may not lead to strong bones.[12] While there are numerous clinical studies demonstrating that calcium supplementation can retard bone loss, the data really is inconclusive regarding a high dietary calcium intake from milk for the prevention of osteoporotic fractures.
One of the most enlightening clues that milk consumption may not be beneficial for bone health is data showing that countries with the highest dairy intake also have the highest rates of hip fracture per capita.[13] Data from a nurses health study involving nearly 80 thousand women, gave an outcome showing no evidence that a higher intake of milk reduced fracture incidence.[14] The most telling facts to come out of this study were that women who drank two or more glasses of milk per day had a relative risk of 45% for hip fracture, compared to women consuming one glass or less per week.
The real take home message seems to be that the more milk consumed, the more likely you are to experience hip fracture. This data supports the hypothesis that not everybody needs milk, and maybe there are other bone structures just as important for bone health. So what could be the problem of milk as a calcium based food source?
Not all Calcium is Created Equal!
Despite the abundance of evidence on the positive influence calcium can have on bone mineral density, pre-menopause calcium from milk and other milk derivatives (yoghurts and cheeses) may not be the most efficient source of calcium. Recent findings from human studies[15,16] have demonstrated that milk calcium (tri-calcium phosphate) is no better absorbed than many other forms of synthetic calcium used in many dietary supplements (carbonate, gluconolacate, citomalate, chloride, lactate, acetate and citrate). In fact, the most readily absorbable form of calcium delivering the largest supply of calcium to your bones is calcium citromalate (CCM),[17] so look out for this on your supplement label. A good tip to test the solubility and absorbability of your calcium supplement is to drop the tablet into vinegar and if it does not dissolve within 30 minutes, you may need to buy another make of supplement.
Despite dairy products not being the best form of calcium delivery, milk is a good source of calcium taken on its own, as it is very similar to the ratio of calcium phosphate found in bone (2:1) – this makes it absorbable (40% of calcium intake from milk is absorbed).[18] The rational behind why we see very little impact of high dairy based diets on bone health may be due to the other foods eaten at the same time.
There are many studies[19,20] that have examined substances in our everyday diet that can bind to calcium making it unavailable for absorption. Two such common binding substances are oxolates (found in many green vegetables and chocolate) and phytates (found in unleavened grain products). Future research into the benefits of dairy products and bone health should take this into consideration, until this time I would advise you rely on dietary souces of calcium rich foods that are low in these compounds such as broccoli, kale and bok choy or other mustard greens.
Beyond Calcium
The final nail in the proverbial coffin of calcium as the holy grail of bone health is that following menopause, calcium cannot be absorbed on its own.[21] Because of this, bone biochemists and associated researchers have raised the issue of importance of other nutrients that are vital for calcium absorption, especially post menopause. Finally, bone is not only composed of calcium but other vital minerals and proteins that contribute to both the process of remodelling and a healthy skeletal system. Although the mineral component is important for bone strength and toughness, the collagen matrix has a profound impact on bone fragility.[22]
Phosphorous
Phosphorous (P) is second to calcium in abundance in the human body, with 85% bound tightly to the human skeleton. Although phosphate is an essential nutrient, there is concern that excessive amounts may be detrimental to bone. For example, rising dietary P increases serum (blood) P and causes a transient fall in Ca resulting in elevated parathyroid hormone secretion and potentially bone resorption (breakdown).[23,24] Dietary P intake has risen some 10-15% over the past 20 years because of the increased use in food additives and cola beverages.[25] Governmental food databases used by many a dietician will not reflect these changes, but in the US adult population, P intake is between 1000-1500mg a day – well above the levels of 700mg currently recommended.
Dietary source: meat, fish, nuts, legumes and cereals.
Magnesium
There are approximately 25 grams of magnesium (Mg) in the human body, with two-thirds located in the skeleton. The Mg in bone is an integral part of hydroxyapatite (the preferred storage form for Ca) formation, and without adequate dietary intake, calcium metabolism is negatively altered. A series of studies carried out in the late 90s have shown Mg deficiency can lead to an uncoupling of bone formation and increased resorption.[26,27] An effective recommended intake is around 300-400mg per day, with data indicating improved BMD in post menopausal women in less than a year.[28]
Dietary source: whole grains, broccoli, nuts and seeds.
Flouride
With the government considering adding fluoride (F) to our drinking water in 2003, the issue of F use is about to heat up over the coming months. The question really is, can sodium fluoride supplementation benefit bone and/or effect bone? There is data to suggest that F is a potent stimulator of osteoblastic bone formation and results generally in an increase in spinal bone mass of circa 5-10% annually.[29] However, very large scale studies, such as the Mayo Clinic[30] study, show that, although elevated bone densities were demonstrated, there was no measurable impact on incidence of fracture rates. My own personal view is to hold back on the use of F for specifically targeting bone health, as the scientific jury is still out regarding its usefulness and also its level of toxicity.
Zinc
The human body contains about 2 grams of zinc (Zn), about 90% of which is found in bone, skin, muscle and hair. Zinc plays a vital role in connective tissue metabolism acting as a cofactor for several enzymes, including alkaline phosphates (necessary for bone mineralization) and collagenase (essential for the development of the collagenous structure of bone).[31] During periods of Zn deficiency, bone levels are greatly reduced – excessive excretion of Zn is related to osteoporosis.[32] Supplementation with Zn has been observed to lead to increased femoral bone mass in conjunction with treadmill exercise.[33] The time for possible supplementation with Zn is during adolescence or for those of us involved in excessive exercise where our levels of Zn may be under stress due to increased rates of growth and/or bone turnover. The current RDA is around 12mg per day but research suggests a level of 30mg is needed for optimal bone health.
Dietary source: meat, fish, oysters, legumes and poultry.
Vitamin D (calciterol)
It may get a lot less publicity than Ca, but vitamin D is just as important for bone health. Where studies show a significant impact of calcium supplementation on BMD, we usually find participants have also received adequate vitamin D intake.
A great aspect of vitamin D is, although we can get it from dietary sources, it has been shown that 15-30 minutes of sun exposure on the hands and face per day is adequate for vitamin D production,[34] thanks to a chemical reaction powered by UV. Vitamin D helps the absorption of calcium from the blood to bone and, as such, deficiency has been shown to play a role in osteoporosis. When deficient Ca is released from bone rather than absorbed, we can see the possible impact this vital nutrient plays in bone health. In a review of 16 studies that assessed hip fracture, the use of 1g of Ca per day decreased the incidence of fracture by 24%. When combined with vitamin D, however, this increased to 54% in some cases.[35] Therefore, the role vitamin D plays in optimal bone health cannot be underplayed and, as such, must be one of the key components of any therapy to treat osteoporosis.
Dietary source: butter, margarine, liver and eggs.
Vitamin K
Vitamin K is a fat-soluable vitamin that exists as K1 in plants but as K2 when formed by human bacteria in the intesting. Its role in bone health is due to the chemical modifications it can exert on osteocalcin, a bone protein vital for bone strength and growth. Low concentrations of vitamin K have been linked to increased risk of hip fracture.[36] Recent studies have demonstrated that supplementation with vitamin K2 in patients becoming non-responsive to HRT significantly increased BMD within 1 year.[37]
Dietary source: broccoli, cabbage, spinach, lettuce.
Ipriflavone
This really is one of my personal favourites at this time for bone health. Ipriflavone is a synthetic form of naturally occurring isoflavones synthesized from the soy isoflavone daidzein. Ipriflavone is beginning to show real promise for its ability to impact BMD. In a study conducted by researchers in Italy, 56 postmenopausal women were given 1g of Ca + 200mg (3 x a day) of ipriflavone or a placebo. After 2 years of treatment, women taking calcium only showed a 5% decline in BMD but there was no loss reported in those taking ipriflavone.[38] Similar data has been shown in a recent study from Japan.[39] This data suggests that ipriflavone suppresses bone resorption, and new research released this year has shown beneficial effects on patients that have undergone ovariectomy and steroid use.[40,41]
Other Nutrients for Bone Health
There are many other food stuffs including soy, PUFAs, vitamins B12 , A and C, and silicone that may play a role in bone health and must be considered. More data is also being released on the negative impact protein can have on Ca release from bone, but the general scientific consensus is inconclusive at best. However, those covered above are at present of most importance and have the largest pools of research to back their claims as successful modulators of bone health.
Exercise & Lifestyle: What Impact on Bone Health?
This article has been primarily aimed toward the use of nutritional interventions via diet or supplementations; however, the impact of exercise and a healthy lifestyle cannot be disregarded. Exercise plays a definitive role in the prevention of osteoporosis. The whole promise of 'use it or lose it' has never been more appropriately applied when it comes to bone health – especially for women. Bones build up in response to physical stress and, as such, breakdown when that stress is no longer there. Regular weight-bearing exercise has been shown to maintain bone mass and in some cases increase it. In a recent report on 580 postmenopausal women, researchers found that increased stair-climbing and walking daily was significantly linked with higher bone mineral densities in the hip and in the entire skeleton.[42] The result is a decrease in both incidence and risk of fracture.
Looking to the negative side of our lifestyle choice, the two nasties are caffeine and smoking. Caffeine has been known for some time to increase urinary loss of Ca. Over the long term its effects may be more damaging, with recent data showing a change in our ability to absorb Ca from the intestine.[43,44] If you are a real coffee fiend, like myself, research has shown that we can offset its detrimental effects in the short term with the addition of 40mg extra a day of Ca (about two tablespoons full of milk). A study released in April 2003 demonstrated that smoking inhibits the action of those important cells involved in bone building, the osteoblasts,[45] and can lead to a significantly greater risk of developing conditions such as osteoporosis in later life.
The Take Home Message
With the prolonged life expectancy of the nation now evident, it is predicted that we will see a greater rise in the incidence of bone disorders including osteoporosis. These conditions can be treated effectively with dietary modifications and a healthier lifestyle. Although the primary aim should always be to achieve peak bone mass in early adulthood, it is never too late to impact bone loss through an integrated nutritional approach. Using a famous quote from Oscar Wilde: "Truth is seldom pure and never simple", but by increasing our awareness of the issues surrounding optimal nutrition, the realization that calcium is really not the only key to healthier, stronger bones will become evident even to the most die hard supporters of calcium supplementation.
Therapeutic Case Study
"Most people describe Basilios Karachalios as 'positive and joyful' participating in many social and cultural activities. However since suffering from osteoporosis he has had to deal with many physiological challenges of the disease. Over the past decade, Mr Karachalios, 67, a retired primary school teacher, continually lost height and had severe spinal pain. In the summer of 1997, he was diagnosed with osteoporosis following radiographs and measurement of spinal bone density. His treatment consisted of calcium supplementation and vitamin D, with exercise to reduce his postural problems and strengthen his muscles. He says, " Now I realize that this disease can be assured and I already feel much better thanks to the treatment, and I look forward to a healthier future".
Exert from: International Osteoporosis Foundation (2003).
Calcium Mythology: Animal Vs Human
"When interpreting data from animal studies to humans there are a few differences that should be taken into account regarding how their body will react to nutritional and pharmacological interventions proposed to effect bone health."
1. The main species studies are rats, pigs, guinea pigs and primates. All have different physiological responses to dietary and drug interventions.
2. Rats have high levels of phytase in their intestines that allow them to hydrolyze/breakdown phyates in food allowing absorption of food in the large intestine. Humans and pigs cannot do this, making the rat an unsuitable model.
3. Rats and guinea pigs nibble and graze continuously without well-defined meal times. Humans and pigs are not like this.
4. Rats have continually growing skeletons, which never reach a bone remodelling stage, unlike humans.
5. Pigs and rats lose very little, if any, calcium from their urine, so make unsuitable models for the study of factors that influence urinary calcium levels in humans. Pigs offset this by and increase in faecal excretion of calcium.
6. Pigs are omnivores and have a diet with a frequency of intake similar to humans and reach a stage of bone remodelling46 making them our closest model of study for osteoporosis in humans.[47]
References
1. The National Osteoporosis Society. Osteoporosis: Causes, prevention and treatment. 3-21. Retrieved may 24th 2003, from http//www.nos.org.uk/public.asp. 2001.
2. Pocock NA, Eisman JA, Hopper JL, Yeates MG, Sambrook PN and Eberl S. Genetic determinants of bone mass in adults. A twin study. J Clin Invest. 80: 706 – 710. 1987.
3. Adachi JD, Bensen WD and Brown J. Intermittent cyclical etidronate therapy in the prevention of corticosteroid-induced osteoporosis. N Engl J Med. 337: 382 – 387. 1997.
4. Montemurro L, Schiraldi G and Fraiolo P. Prevention of corticosteroid induced osteoporosis with salmon calcitonin in sarcoid patients. Calcif Tissues Int. 49: 71 – 76. 1991.
5. Yoneda K, Tanji Y, Ikeda N, Miyoshi Y, Taguchi T, Tamaki Y and Noguchi S. Influence of adjuvant tamoxifen treatment on bone mineral density and bone turnover markers in postmenopausal breast cancer patients in Japan. Cancer Lett. 186 (2): 223 -230. 2002.
6. Hernandez E, Valera R, Alonzo E, Bajares-Lilue M, Carlini R, Capriles F, Martinis R, Bellorin-Font E and Weisinger JR: Effects of raloxifene on bone metabolism and serum lipids in post monopauseal women on chronic hemodialysis. Kidney Int. 63(6): 2269 – 2274. 2003.
7. Neele SJ, Evertz R, De Valk-De Roo G, Roos JC and Netelenbos JC. Effect of 1 year of discontinuation of raloxifene or oestrogen theraphy on bone mineral density after 5 years of treatment in healthy postmenopausal women. Bone. 30(4): 599 – 603. 2002.
8. Rohatgi N, Blau R and Lower EE. Raloxifene is associated with less side effects than tamoximen in women with early breast cancer: a questionnaire study from one physician's practice. J Womens Health Gend Based Med. 11(3): 291 – 301. 2002.
9. Grady D, Herrington D, Bittner V, Blumenthal R, Davidson M, Hlatky M, Hsia J, Hulley S, Herd A, Khan S, Newby LK, Waters D, Vittinghoff E and Wenger N: Cardiovascular disease outcomes during 6.8 years of hormone therapy: Heart and oestrogen/progestin replacement study follow-up (HERS II). 288(1): 49 -57. 2002.
10. Vogelvang TE, Mijatovic V, Kamp O, Netelenbos JC, Neele SJ, Pines A, Kenemans P and van der Mooren MJ. Neither long-term treatment with raloxifene nor hormone replacement therapy modulate cardiac function in healthy postmenopausal women: two randomised, placebo-controlled, 2-year studies. Am J Obstet Gynocol. 186(4): 729 – 736. 2002.
11. Olsson HL, Ingvar C and Baldstrom A: Hormone replacement therapy containing progestins and given continuously increases breast carcinoma risk in Sweden. Cancer. 97(6): 1387 – 1392. 2003.
12. Feskanich D, Willett WC and Coiditz GA. Calcium, vitamin D, milk consumption, and hip fractures: a prospective study among postmenopausal women. Am J Clin Nut. 77(2): 504 – 511. 2003.
13. Smith R. Epidemiologic Studies of Osteoporosis in Women of Puerto Rico and Southeastern Michigan with Special Reference to Age, Race, National Origin, and to Other Related or Associated Findings. Clin Orthop. 45: 31-48. 1966.
14. Feskanich D, Willett WC and Coiditz GA. Calcium, vitamin D, milk consumption, and hip fractures in women: a 12-year prospective study. Am J Pub Health. 87: 992 – 997. 1997.
15. Recker RR, Bammi A, Barger-Lax MJ and Heaney RP: Calcium absorbability from milk products, imitation milk, and calcium carbonate. Am J Clin Mutr. 47: 93 – 95. 1988.
16. Smith TM, Kolars JC, Savaiano DA and Levitt MD. Absorption of calcium from milk and yogurt. Am J Clin Nutr 42. 1197 – 1200. 1985.
17. Heaney RP, Recker RR and Weaver CM. Absorbability of calcium sources: The limited role of solubility. Calcif Tissue Int 46: 300 -304. 1990.
18. Gueguen L and Pointillart A. Biovailability of dietary calcium. J Am Coll Nutr. 19(2): 1195 – 1365. 2000.
19. Allen LH. Calcium bioavalibility and absorption: a review. Am J Clin Nutr. 35: 783 – 808. 1982.
20. Pointillart A and Gueguen L. Influence des fibres alimentaires sur la biodisponibilite des mineraux. Cah ENSBANA. 8: 157 – 182. 1992.
21. Wishart JM, Scopacasa F, Horowitz M, Morris HA, Need AG, Clifto PM and Nordin BE. Effect of perimenopause on calcium absorption: a
longitudinal study. Climacteric. 3(2): 102 – 108. 2000.
22. Young MF. Bone matrix proteins: their function, regulation and relationship to osteoporosis. Osteoporos Int. 12: 35 – 42. 2003.
23. Calvo MS, Kumar R and Heath H. Elevated secretion and action of parathyroid hormone in young adults consuming a high phosphorus, low calcium diets assembled from common foods. J Clin Endocrinol Metab. 66: 823 – 829. 1988.
24. Calvo MS, Kumar R and Heath H: Persistently elevated parathyroid hormone secretion and action in young women after 4 weeks of ingesting phosphrous, low calcium diets. J Clin Endocrinol Metab. 70: 823 – 1334, 1340. 1990.
25. Petridou E, Karpathios T, Dessypris N, Simou E and Trichopoulos D. The role of dairy products and non-alcoholic beverages in bone fractures among school age children. Scand J Soc Med. 25: 119 – 125. 1997.
26. Rude RK, Kirchen ME, Gruber HE, Meyer MH, Luck JS and Crawford DL. Magnesium deficiency induces bone loss in the rat. Miner Electrolyte Metab. 24: 314 – 320. 1998.
27. Rude RK, Kirchen ME, Gruber HE, Meyer MH, Luck JS and Crawford DL. Magnesium deficiency-induces osteoporosis in the rat: Uncoupling of bone formation and bone resorption. Magnes Res. 12: 257 – 267. 1999.
28. Abraham GE and Grewal H. A total dietary program emphasizing magnesium instead of calcium. Effect on the mineral density of calcaneous bone in post menopausal women on hormonal therapy. J Reprod Med. 35: 503 – 507. 1990.
29. Resch H, Libanati C, Farley S, Bettica P, Schultz E and Baylink DJ. Evidence that fluoride therapy increases trabecular bone density in a peripheral skeletal site. J Clin Endocrinol Metab. 76: 1622 – 1624. 1993.
30. Riggs BL, Hodgson SF, O'Fallon WM, Chao EY, Wahner HW, Muhs JM, Cedel SL and Melton LJD. Effect of fluoride treatment on the fracture rate in postmenopausal women with osteoporosis. N Eng J Med. 322: 802 – 809. 1990.
31. Beattie J and Avenell A. Trace element nutrition and bone metabolism. Nutr Res. 5: 167 – 188, 1992.
32. Calhoun NR, Smith Jr JC and Becker KL. The role of zinc in bone metabolism. Clin Orthop. 20: 212 – 234. 1974.
33. Seco C Revilla M, Hernandez ER, Gervas J Gonzalez-Riola J, Villa LF and Rico H. Effects of Zinc supplementation on vertebral and femoral bone mass in rats on strenuous treadmill training exercise. J Bone Miner Res. 13: 508 – 512. 1998.
34. Sayre RM, Dowdy JC, Shepherd J, Sadig I, Bager A and Kollias N. Vitamin D production by natural and artificial sources. Orlando, Florida, Photo Medical Society Meeting. 3-1-1998. Ref Type: Conference Proceeding. 1998.
35. Reid IR. The roles of calcium and vitamin D in the prevention of osteoporosis. Endocrinol Metab Clin North Am. 27(2): 389 – 398.
36. Kanai T, Takagi T, Masuhiro K, Nakamura M, Iwata M and Saji F: Serum vitamin K level and bone mineral density in postmenopausal women. Int J Gynaecol Obstet. 56: 25 – 30. 1997.
37. Hidaka T, Hasegawa T, Fujimura M, Sakai M and Shigeru S. Treatment for patients with postmenopausal osteoporosis who have been placed on HRT and show a decrease in bone mineral density: effects of concomitant administration of vitamin K2. J Bone Min Metab. 20(4): 235 – 239. 2002.
38. Gennari C, Agnusdei D, Crepaldi G, Isaia G, Mazzuoli G, Ortolani S, Bufalino L and Passeri M. Effect of ipriplavone – a synthetic derivative of natural isoflavone – on bone mass loss in early years after menopause. Menopause. 5 (1): 9 – 15. 1998.
39. Ohta H, Kuroda K, Mafune Y, Yoshida T, Kamimura T, Aiba T and Ishihara N. Effect of 1 year ipriflavone treatment on lumbar one mineral density and bone metabolism markers in postmenopausal women with low bone mass. Hormone Res. 51: 178 – 183. 1999.
40. Katase K, Kato T, Hirai Y, Hasumi K and Chen JT. Effects of ipriflavone on bone loss following a bilateral ovariectomy and menopause: a randomised placebo – controlled study. Calcif Tissue Int. 69(2): 73 – 77. 2001.
41. Head KA. Ipriflavone: an important bone-building isoflavone. Altern Med Rev. 4(1): 10 – 22. 1999.
42. Coupland CA, Cliffe SJ, Bassey EJ, Grainge MJ, Hosking DJ and Chilvers CE. Habitual physical activity and bone mineral density in postmenopausal women in England. Int J Epidemiol. 4(2): 241 – 246. 1999.
43. Rapuri PB, Gallagher JC, Kinyamu HK and Ryschon KL. Caffeine intake increases the rate of bone loss in elderly women and interacts with vitamin D receptor genotypes. Am J Clin Nutr. 74(5): 694 – 700. 2001.
44. Heaney RP. Effects of caffeine on bone and the calcium economy. Food Chem Toxicol. 40(9): 1263 – 1270. 2002.
45. Liu X,Kohyama T, Kobayashi T, Abe S, Kim HJ, Reed EC and Rennard SI. Cigarette smoke extract inhibits chemotaxis and collagen gel contraction mediated by human bone marrow osteoprogenitor cells and osteoblast-like cells. Osteoporos Int. 14: 235 -242. 2003.
46. Scholz-Ahrens KE, Delling G, Jungblut PW, Kallweit E and Barth CA. Effect of overectomy on bone histology and plasma parameters of bone metabolism in nulliparus sows. Z Ernahrungswiss. 35: 13 – 21. 1996.
47. Bartlet JP, Coxham V, Davicco MJ and Gaumet N. Animal models for postmenopausal osteoperosis. Reprod Nutr Dev. 34: 221 – 236. 1994.
Comments:
-
No Article Comments available