Positive Health Online
Your Country

![[Image: https://www.water-for-health.co.uk/]](/img/original/BannerAvatar/4046.12831f50177f8848ee87b8e94411d6b3.jpg "https://www.water-for-health.co.uk/")
![[Image: http://www.abundanceandhealth.co.uk]](/img/original/BannerAvatar/2836.df7d2315253110ff5b3a566f94871f99.jpg "http://www.abundanceandhealth.co.uk")
![[Image: https://peacegifts.shop/]](/img/original/BannerAvatar/3906.e1d1ebc07ce7530bbb3d6cf426966b6f.jpg "https://peacegifts.shop/")
![[Image: http://www.balens.co.uk]](/img/original/BannerAvatar/2148.50367fa908013fae0a7f1a171543ef92.jpg "http://www.balens.co.uk")
![[Image: http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer]](/img/original/BannerAvatar/1859.1296090fd8385e7ceff51c8011559097.jpg "http://www.drsgoodman.com/books-goodman/52-nutrition-and-cancer")
![[Image: IFPA Int'l Fed Aromatherapists]](/img/original/TopicbannerAvatar/1185.9b7a831d484259621c55f48bd9933c3a.jpg "IFPA Int'l Fed Aromatherapists")
![[Image: ICAN International Clinical Aromatherapy Network]](/img/original/TopicbannerAvatar/4442.566a83a07de79de73b9c738f7fb6458a.jpg "ICAN International Clinical Aromatherapy Network")
![[Image: ISNS International Science and Nutrition]](/img/original/TopicbannerAvatar/4310.3fe1bd582f0b1b36c39fca00e3464581.jpg "ISNS International Science and Nutrition")
![[Image: Organic Aromatherapy]](/img/original/TopicbannerAvatar/1001.12a011c5d14492e86a5a2fa985244b74.jpg "Organic Aromatherapy")
The Effect of Aromatherapy Treatment on Raised Arterial Blood Pressure
listed in aromatherapy, originally published in issue 39 - April 1999
Aromatherapy treatment is widely used for the purpose of relaxation and although the effects of aromatherapy massage are controversial, there is a shortage of controlled studies to substantiate its beneficial effect on the raised arterial blood pressure. The literature published in the last few years primarily concerns itself with acupuncture, homeopathy, spinal manipulation and herbalism (Department of Complementary Medicine, University of Exeter – 1997 publications). However, there are reported cases of successful treatment of gestational hypertension using oils such as rosewood (McArdle, 1992). Rosewood was also used by Waymouth (1992) for essential hypertension.

At the Natural Health Centre in Preston, Lancashire, England
I decided with my supervisor that it was not possible to arrange a double-blind study using only aromatherapy massage as an alternative because of their action on the olfactory nerve. Due to their easily recognisable smell, not only the therapist, the observer and the supervisor would recognise the intervention, the patients would be aware of it as well. Blinding, therefore, was very difficult. The treatment group subjects were to receive massage with pure essential oils and the control group were to receive the same treatment but only with the carrier oil.
Another difficulty arose in an objective evaluation of the effects of individually blended pure essential oils for each individual patient in the treatment group. It was also found that difficulty developed in an objective evaluation of pain and relaxation.
It was hoped that this pilot study in effect will form the basis for a future large-scale research on the effect of aromatherapy massage on the raised arterial blood pressure.
Abstract
The selection of twenty subjects was based on the reading of blood pressure above the average of 140/80 mmHg in each case. The blood pressure was taken before and after each treatment on the same arm with the same sphygmomanometer. Patients were not on medication and allocation of subjects to either the control group or the treatment group was conducted by tossing a coin and placing the results in twenty sealed, sequentially numbered envelopes coded A1 to A10 (treatment group) and BM1 to BM10 (control group). The subjects were to receive five treatments over a period of six weeks. The protocol for the study was acknowledged by the Local Ethics Committee in Preston.
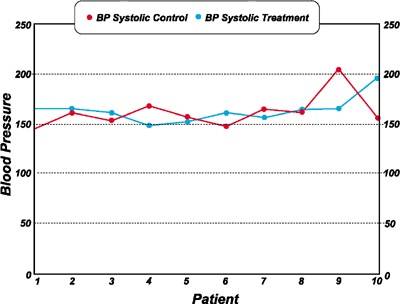
Before: Comparison of systolic blood pressure in treatment of control groups
After: Comparison of systolic blood pressure in treatment of control groups
Patients received treatment of 45 minutes duration using the same carrier oil and the same technique of massage. They were treated by the same therapist and their appointments were booked in advance for the same day of the week and the same time of the day. The same treatment room was allocated for each individual throughout the study and procedure of each appointment followed the same pattern each time.
Patients were advised that they would receive tactile treatment, but no further details were revealed at this stage so the subjects were not informed to which group they would have been allocated. This approach was adopted following advice of the Chairman of Local Research Ethics Committee.
A questionnaire was introduced during the pilot study after the first treatment and subjects were asked to fill in the last one at home after the fifth treatment. They were asked to post it to the Natural Health Centre in the self-addressed envelope provided, one week after their last treatment.
The study took place over March and April in 1998. In an attempt to reduce examiner bias, the patients forms were filled in by the patients along with a consent from and an explanatory letter was given to each patient by the examiner.
It was considered by the researcher to be truly ethical if treatments were rendered free of charge hence subjects were not paying for the received treatments and the pilot study, therefore, was based on a more professional basis.
Study Population
Ten patients were allocated to the control group and the treatment group. The first pre-treatment consultation forms were filled in by each patient before treatment and before the patient had met the practitioner. All patients taking part in the trial filled in the questionnaires at the beginning of their consecutive treatment and all patients filled in the same self-addressed questionnaires at the end of the clinical trial on the seventh day from their last, fifth treatment and posted them to the clinic. All questionnaires have been completed and returned.
Methodology
It was felt that it was not possible to set this pilot study on a randomised clinical trial (RCT) basis. It was also felt that it was difficult to set up a study where each individual subject would receive an individually blended pure essential oils for each individual treatment.
The raised systolic blood pressure may be the result of different internal and external factors contributing to the causation of the raised diastolic blood pressure. Therefore, depending on the cause and extension of the blood pressure reading there would be a need for application of different pure essential oils. Also, essential oils would need to be matched with the personality and the state of health (mental and physical) and body weight of a patient at the time of treatment. In other words, the assessment as to the appropriate use of the most beneficial essential oils would need to be assessed on an individual basis to fit the Holistic Medical Model approach of the character of natural medicine. For this study, it was decided to use only three pure essential oils of ylang-ylang, clary sage and marjoram.
Sampling
A non-random method of sampling was employed for the purpose of this study. It was aimed to sample a group of people with a particular characteristic, namely raised arterial blood pressure. This method is used primarily in qualitative research design. In the study, it was also used in order to pilot the questionnaire.
The sampling was also purposive in nature in order to generate hypotheses for further study and it was used for practical reasons because the study was conducted on a small scale basis, but in the case of a large scale clinical trial, random sampling may be possible because the re-selection of patients may not be of great importance. Snowballing technique of sampling was partly employed for this study since patients taking part had to display blood pressure readings above 140/80 mmHg.
The randomised control trial (RCT) protocols are very often not applicable in clinical research when intervention such as the tactile treatment is involved. The Holistic Medical Model of natural medicine virtually precludes the use of strict application of scientific research methods as we know them.
Materials and Methods
The pure essential oils used for this pilot study were:
Ylang-ylang
(Cananga odorata) for its content of alcohols and the cadinene which are hypotensive (Tiran 1996). Ylang-ylang is renowned as a treatment for emotionally related conditions such as nervous tension, arterial hypertension, tachycardia and palpitations (Rose, 1994).
Clary sage
(Salvia sclarea) for its analgesic and antispasmodic actions and stress-related problems (Tiran, 1996). Clary sage can decrease heart rate (Buckle, 1997) and according to Rovesti and Gattefosse (1973) Clary sage is mildly hypotensive.
Marjoram
(Origanum marjorana) for its properties helping to combat anxiety and stress. Aldehydes, in the form of citral and geranyl acetate, add to the anti-infective qualities and also lower the blood pressure (Tiran, 1996).
The carrier oil used as lubricant in the study was an unrefined grapeseed oil. The blend consisted of 15ml of unrefined grapeseed oil and one drop of each of the pure essential oils of Ylang-ylang, Marjoram and Clary sage. A fresh blend of massage medium was being prepared prior to each treatment and blending was supervised by the author.
Questionnaire and Validity
Much of the work took place at the questionnaire design stage. It was agreed that the questionnaire should take a simple format and be quick to fill in. It was a two-sided form, consisting of a mixture of open and closed questions. There was not enough time to formally pilot the questionnaire prior to the study. However, it was tested for a two week period on colleagues and willing fee-paying patients attending their regular treatment sessions at the Natural Health Centre in Preston.
Massage Technique
Five elemental techniques were used in body massage employed in this study: effleurage (stroking), petrissage (kneading), gentle friction, vibration and feathering. The whole body massage was initiated with effleurage, progressing to petrissage, friction and vibration – culminating in effleurage and feathering (Basnyet 1997; Prentice 1990). Massage routinely progressed from distal to proximal body parts.
Results
There were eight females and two male patients in the treatment and the control groups. The majority of patients had raised arterial blood pressure of longer than a calendar year in duration; three patients in the treatment group suffered from high blood pressure for over 5 years, only one patient in the control suffered from raised arterial blood pressure for over 5 years.
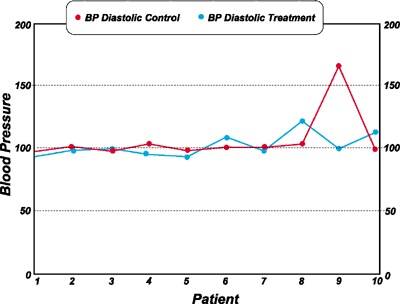
The average initial blood pressure reading in the treatment group was 163/102 mmHg and in the control group this reading averaged to 162/106 mmHg.
The average last blood pressure reading in the treatment group was 132/78 mmHg and in the control group 149/93 mmHg.
The lowest blood pressure reading after last aromatherapy treatment was 130/84 mmHg and the respective lowest reading in the control group was 136/90 mmHg.
The highest initial pulse rate reading before the initial treatment in the treatment group was 104 (the lowest reading was 47) and in the control group it was 88 (the lowest reading being 62). The highest initial pulse rate reading of 104 came down to 87 after last treatment in the treatment group and the highest initial pulse rate reading of 88 came down to 76 in the control group after the last treatment. The difference of 17 and 12 respectively.
Questionnaire
All respondents noticed a change in the way they felt after each treatment. The feeling of relaxation was felt for 6 days after last treatment in the treatment group and 5 days in the control group.
70% of patients in the treatment group reported a noticeable improvement in duration of their pattern of sleep and 50% in the control group. 80% of treatment group subjects reported improved quality of sleep and 50% of the control group.
100% of treatment group patients observed improved breathing and 80% of the control group noticed positive effect of treatment.
90% of patients in the treatment group noticed improvement in blood circulation in the extremities and only 50% acknowledged positive effect in the control group.
A self-assessed feeling of improvement on a scale of 1 to 10 started from 3 in the treatment group whereas the control group improvement was more gradual and started from 1. The treatment group patients recorded greater improvement in their own assessment than patients in the control group.
Discussion
The raised blood pressure was reduced in 7 cases in the treatment group and in 6 cases in the control group. It has to be emphasised that the improvement in the pulse rate was consistently greater in the treatment group than in the control group.
The most significant change in the treatment group was one case of blood pressure measurement before the first treatment of 196/112 mmHg as compared to 165/98 mmHg at the last (after treatment) blood pressure reading.
In one subject in the treatment group blood pressure reading of 205/165 mmHg went down to 176/97 mmHg at the last (after treatment) reading. The systolic blood pressure decreased gradually by 29 and diastolic by 68 at the end of the study.
Ten subjects in the treatment group reported improvement in their general state of health and nine subjects were positive in their self-assessment in the control group.
Conclusion
All participating subjects in both groups stated in the questionnaire that they benefited from the treatment. It would be possible in a large-scale study, to use individually selected pure essential oils according to the reasons of raised blood pressure and according to the body weight, say four drops of the chosen oils instead of three drops and over a longer period of time. There are several other pure essential oils which could have been used in the blends and carrier oils such as Vitamin E or Evening Primrose could have been used in the carrier oil. All these factors could have been applied in a variety of blends differing from one treatment to another and from one subject to another.
The result of this study confirmed positively the gradual improvement in the measurements of the blood pressure readings. Greater improvement was achieved in the subjects allocated to the treatment group. However, overall blood pressure readings in both groups improved successfully, which would indicate that this type of tactile treatment can have a beneficial effect on the raised arterial blood pressure.
Bibliography - List of References
Arcier, M. (1992): Aromatherapy. London, Hamlyn.
Arnould-Taylor, W. (1997): Principles & Practice of Physical Therapy, 4th edn. London, Stanley Thornes (Publishers) Ltd.
Balacs, T. (1991b): Research reports. Int J Aromatherapy 3(4): 20-31.
Balacs, T. (1993): Research reports. Int J Aromatherapy 5(3): 34.
Balacs, T. and Tisserand, R. (1995): Essential oil safety. London, Churchill Livingstone.
Barr, J.S. & Taslitz, N. (1970) The influence of back massage on autonomic functions. Phys Ther 50(12): 1679-1691.
Basnyet, J. (1997): Massage, London, Salamander Books Ltd.
Bowling, A. (1997): Research Methods in Health. Buckingham, Open University Press.
Buchbauer, G., Jirovetz, L:. and Jager, W. (1993): Fragrance compounds and essential oils with sedative effects upon inhalation. Journal of Pharmaceutical Sciences 82, 660-64.
Buccellato, F. (1982): Ylang survey. The Perfumer and Flavorist 7, 9-10.
Buckle, J. (1993): Aromatherapy. Does it matter which lavender essential oil is used? Nursing Times 89(20): 32-35.
Buckle, J. (1997): Clinical aromatherapy in nursing. London, Arnold (Hodder Headline Group).
Clark, P.E., Clark, M. (1984): Therapeutic touch: Is there a scientific basis for the practice? Nursing Research 31(3): 37-41.
Cruz-Coke, R. (1960): Environmental influences and arterial blood pressure. Lancet 345, 295-6.
Cyriax, J., Russell, G. (1980): Textbook of orthopaedic medicine (Vol 2, 10th ed). Baltimore, Williams & Wilkins.
D.E. & Morelli M. (1991): Effects of massage on motorneuron excitability. Phys Ther 71(8): 555-560.
Dunn, C., Sleep, J. and Collett, D. (1995): Sensing an improvement: an experimental study to evaluate the use of aromatherapy, massage and period of rest in an intensive care unit. Journal of Advanced Nursing 21, 34041.
Gattefosse, M. (1992): Gattefosse's aromatherapy (translated by Tisserand, R). Saffron Walden, C W Daniel.
Ginsberg, F. & Famaey, J.P. (1987): A double-blind study of topical massage with Rado-salil ointment in mechanical low-back pain. J Int Med Res 15: 148-153.
Gobel, H., Schmidt, G. and Soyka, D. (1994): Effect of peppermint and eucalyptus oil preparations on neurophysiological and experimental algesimetric headache parameters. Cephalagia 14, 228-34.
Guenther, E. (1972: The essential oils. Malabar, FL:Krieger.
Hardy, M., Kirk-Smith, M.D.and Stretch, D.D. (1995): Replacement of drug treatment for insomnia by ambient odour (letter). Lancet 346, 701.
Imberger, I., Rupp, J., Daramat, C. & Buchbauer, G. (1993): Effects of essential oils on human attentional processes. Programme Abstracts - 24th International Symposium on Essential Oils.
International School of Aromatherapy (1993): A Safety Guide on the Use of Essential Oils. London, Natural by Nature.
Kaada, B., Torsteinbo, O. (1989): Increase of plasma beta-endorphins in connective tissue massage. Gen Pharmac 20, 487-489.
Keller, E., Bzdek, V.M.(1986): Effects of therapeutic touch on tension headache pain. Nursing Research 35(2): 101-105.
Karamat, E., Imberger, J., Buchbauer, G. et al. (1992): Excitatory and sedative effects of essential oils on human reaction time performance. Chem Senses 17(4): 847.
Kirk-Smith, M. & Stretch, D. (1994): Clinical trials in aromatherapy. Int J Aromatherapy 6(1): 32-35.
Krieger, D. (1980): The therapeutic touch. Englewoord Cliffs, Prentice-Hall Inc.
Kuprian, W. (Ed) (1982): Physical therapy for sports. Philadelphia, W B Saunders.
Lavabre, M. (1990): Aromatherapy workbook. Vermont, Healing Arts Press.
Lawless, J. (1997): The illustrated guide to aromatherapy. Dorset, Element Books Ltd.
Lawless, J. (1992): The Encyclopaedia of Essential Oils. Shaftesbury: Element.
Lis-Balchin, Dr M. (1995): Aroma science - the chemistry and bioactivity of essential oils. Surrey, Amberwood Publishing Ltd.
Mastro, B. (1986): Course content: Hawaiian acupressure massage therapy. Altanta, GA: Center for Life.
Metcalfe, J. (1989): Herbs and aromatherapy. Devon, Webb & Bower (Publishers) Ltd.
Prentice, W.E. (1990): Therapeutic modalities in sports medicine (2nd ed.). St. Louis, Times Mirror/Mosby.
McArdle M. (1992): Rosewood in preeclampsia. International Journal of Aromatherapy 4(1): 3 (letter).
Price, S. (1992): The position of aromatherapy in European countries other than Britain. Aromatherapy World, Summer 1992: pp.16-17.
Price, S. (1993): The aromatherapy workbook. Wellingborough, Thorsons.
Price, S. (1995): Aromatherapy for the health professional. London, Churchill Livingstone.
Puustjarvi, K., Airaksinen O. & Pontinen P.J. (1990): The effects of massage in patients with chronic tension headache. Acupuncture and Electrotherapeutics Research Int 15: 159-162.
Roberts, R. (1991): Preventing PPD after surgery. Nursing 4, 28.
Rose, J. (1994): Guide to essential oils. San Francisco, CA. Jeanne Rose Aromatherapy.
Rowe, L. (1989): Anxiety in a coronary care unit. Nursing Times 45, 61-3.
Ryman, D. (1990): The aromatherapy handbook - the secret healing power of essential oils. Saffron Walden, W C Daniel.
Ryman, D. (1991): Aromatherapy - the encyclopaedia of plants and oils and how they help you. London, Judy Piatkus (Publishers) Ltd.
Sellar, W. (1992): The directory of essential oils. Saffron Walden, C W Daniel.
Stevenson, C. (1994): The psychophysiological effects of aromatherapy massage following cardiac surgery. Complementary Therapies in Medicine 2, 27-35.
Tappan, F.M. (1980): Healing massage techniques. Reston VA, Prentice-Hall Inc.
Tiran, D. (1996): Aromatherapy in midwifery practice. London, Bailliere Tindall.
Tisserand, R. (1994): The art of aromatherapy. Saffron Walden, The C W Daniel Co Ltd.
Tisserand, R. and Balacs, T. (1995): Essential oil safety. London, Churchill Livingstone.
Tisserand, R. (1990): The essential oil safety data manual. Sussex, Tisserand Aromatherapy Institute.
Waymouth, S.(1992): Case study - Essential hypertension. Int J Aromatherapy 4(3): 29.
Waterlow, J. (1988): Prevention is cheaper than cure. Nursing Times 84, 69-71.
Williams, D. (1989): Lecture notes on essential oils. London, Eve Taylor Ltd.
Wood, E. (1981): Beard's massage. Philadelphia, W B Saunders Co.
Wren, R.C. (1998): Potter's new cyclopaedia of botanical drugs and preparations. London, Churchill Livingstone.
Valnet, J. (1993): The practice of aromatherapy. Saffron Walden, C W Daniel.
Comments:
-
No Article Comments available